

Volume 14, Issue 1 (Winter 2026)
Iran J Health Sci 2026, 14(1): 25-34 |
Back to browse issues page


Ethics code: IR.MAZUMS.REC.1400.615
Clinical trials code: IR.MAZUMS.REC.1400.615
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kalteh H, Etemadinezhad S, kalteh A, Mousavinasab S, Heidari H, ramzani S. Structural Equation Modeling of Work Ability in Iranian Healthcare Workers: Direct and Indirect Effects of Job Demands and Leadership Through Job Satisfaction and General Health. Iran J Health Sci 2026; 14 (1) :25-34
URL: http://jhs.mazums.ac.ir/article-1-1013-en.html
URL: http://jhs.mazums.ac.ir/article-1-1013-en.html
Hajiomid Kalteh 

 , Siavash Etemadinezhad * , Azimeh Kalteh , Seyed-Nouraddin Mousavinasab , Hamidreza Heidari , Solale Ramzani
, Siavash Etemadinezhad * , Azimeh Kalteh , Seyed-Nouraddin Mousavinasab , Hamidreza Heidari , Solale Ramzani
, Siavash Etemadinezhad * , Azimeh Kalteh , Seyed-Nouraddin Mousavinasab , Hamidreza Heidari , Solale Ramzani
Department of Occupational Health Engineering, Health Science Research Center, Faculty of Health, Mazandaran University of Medical Science, Sari, Iran. , dr.setemadi@yahoo.com
Keywords: Job demands, Leadership, Job satisfaction, General health, Work ability index (WAI), Healthcare workers
Full-Text [PDF 1139 kb]
(120 Downloads)
| Abstract (HTML) (253 Views)
Full-Text: (43 Views)
Introduction
Work ability (WA) was initially conceived in the 1980s by the Finnish Institute of Occupational Health to evaluate workplace health and age-related work capacity [1]. It reflects the balance between individual resources and job demands, encompassing physical and mental capacities, work characteristics, and future ability to meet job requirements [2].
WA is a multifactorial construct influenced by numerous individual and occupational factors. Prior reviews have identified a wide variety of antecedents, including physical, mental, emotional, and psychosocial job demands; work conditions; job resources; job control; fairness; and job security, as well as demographic characteristics, health status, and lifestyle factors [3-5].
Although initial efforts have been made to examine factors influencing WA, the mechanisms through which organizational and psychosocial variables jointly shape WA remain insufficiently understood. Most prior studies have investigated these factors separately, limiting the development of integrated explanatory models [5].
Theoretical frameworks such as lifespan development [6], job demand-resources [7], and job demand-control [8] provide useful foundations for understanding WA, proposing that job demands contribute to health impairment while job resources, including supportive leadership, enhance motivation and work ability [9]. The job demands-resources (JD-R) model stands out as a particularly comprehensive and flexible framework [8]. However, existing empirical research rarely incorporates these theoretical elements into a single comprehensive structural equation model that captures the direct and indirect interactions among job demands, leadership, job satisfaction, and general health [3].
Healthcare workers face high emotional labor, role ambiguity, heavy workload, and continuous exposure to human suffering, all of which may influence WA. Numerous studies have examined the association between WA and physical/mental/psychosocial job demands [10-12]. However, these findings are mixed, likely due to differences in job contexts, variations in how job demands are defined, and the influence of moderating organizational factors [13]. Leadership and job satisfaction have also been identified as relevant psychosocial variables, with evidence suggesting that effective leadership enhances job satisfaction and may indirectly support WA [14, 15]. Nevertheless, the mediating roles of job satisfaction and general health remain theoretically underdeveloped and empirically under examined within comprehensive structural equation models based on the JD-R framework [16].
Given these limitations, there is a clear need for integrated models that simultaneously assess organizational, psychosocial, and individual variables to clarify their combined direct and indirect effects on WA. Such comprehensive analyses are particularly scarce in non-Western settings and among healthcare workers. Therefore, the present study develops and tests a comprehensive structural equation model fully grounded in the JD-R model. This study aimed to explore and test the pathways between psychosocial factors and work ability among Iranian healthcare workers. Data were analyzed using structural equation modeling (SEM) to examine the direct and indirect effects of psychosocial factors, including job demands, leadership, job satisfaction, and general health. The study focused on psychosocial factors within the JD-R framework rather than a comprehensive structural model.
Materials and Methods
The participants in this cross-sectional study were employees of township healthcare centers in northern Iran. A stratified random sampling method was used to ensure representativeness across different healthcare units. Stratification was based on the type of healthcare unit (clinics, hospitals, and rural and urban healthcare centers) to ensure proportional representation from each unit. Within each stratum, the participants were randomly selected from the list of eligible healthcare professionals, including nurses, physicians, midwives, and allied health staff. The number of participants in each stratum was determined proportionally to the size of the unit to maintain representativeness.
The inclusion criteria were clearly defined as healthcare practitioners directly engaged in patient care or healthcare delivery, including nurses, physicians, midwives, and allied health staff, with at least 1 year of work experience. The exclusion criteria comprised administrative personnel, office staff, accountants, cleaning workers, and others not directly engaged in healthcare provision. As the health centers include various medical and health departments (healthcare clinics, hospitals, and rural and urban healthcare centers), only eligible healthcare workers meeting these criteria were included. Out of 579 invited participants, 579 completed the questionnaire and were included in the analysis (response rate: 100%). Non-response bias was therefore not applicable. All participants met the inclusion criteria of becoming healthcare practitioners intimately engaged in patient care or healthcare service delivery. A self-administered questionnaire was used to gather data on demographic and job-related characteristics (age, job experience, job type, and gender) and study variables. Before data collection, the study objectives were clearly explained, and Informed consent was acquired from all individuals.
Psychosocial factors and general health
To assess job demands, leadership status, job satisfaction, and general health, items from the second version of the Copenhagen psychosocial questionnaire (COPSOQ II) were used. The COPSOQ II, as a multi-theory-based instrument, is appropriate for a wide range of analytical levels. The psychometric properties of the COPSOQ have been validated across multiple languages [17]. We used selected subscales from COPSOQ II, specifically the emotional job demand dimension and items reflecting quantitative workload, to focus on the most relevant aspects of job demands affecting healthcare workers in this context [18]. Although the official, validated Persian version does not include a formal “quantitative demands” dimension, these items were adapted from prior literature and contextualized to reflect the most significant workload intensity and emotional challenges faced by healthcare professionals [19].
Other dimensions of COPSOQ II were not included to reduce participant burden and because they were deemed less critical for the current study’s aims. The reliability of the Persian version was verified, with a Cronbach α ranging from 0.75 to 0.89 [20]. Some items included “How often do you not have time to complete all your work tasks?”, “Is your work unevenly distributed so it piles up?”, and “Is your work emotionally demanding?” A 5-option scoring system was used to rate responses (1=always; 2=often; 3=sometimes; 4=seldom; 5=never or hardly ever). Leadership quality was assessed using 4 items, with each person directly evaluating their manager. The items included “Makes sure that the individual member of staff has good development opportunities,” “Gives high priority to job satisfaction,” “Is good at work planning?”, and “Is good at solving conflicts?” The items were rated on a 5-point Likert scale ranging from 1 (to a very small extent) to 5 (to a very large extent). Job satisfaction was measured by considering participants’ perspectives on future job prospects, the physical condition of the work environment, and the use of their skills. Participants rated their satisfaction on a scale from “very dissatisfied” to “very satisfied.”
Furthermore, a single-item scale was used to assess general health, in which participants rated their overall health. The response options ranged from “excellent=1” to “poor=5.” We acknowledge that using a single-item measure may limit psychometric robustness for latent variable modeling. However, evidence from prior studies indicates that single-item measures of health can serve as valid and reliable proxies for general health in epidemiological and occupational health research [21], and limitations are discussed in the manuscript.
Work ability
Despite the availability of numerous instruments to assess work ability, the work ability index (WAI) has been employed more extensively. The WAI is the product of a multidisciplinary team encompassing psychology, physiology, medicine, biostatistics, and epidemiology [22]. The WAI comprises 60 items organized into 7 dimensions: current WA relative to a lifetime best, WA in relation to the demands of the job, amount of physician-diagnosed diseases (indicated by the participant on a checklist of 50 potential diseases), evaluation of impairment resulting from disease or injury, total sick leave days accrued in the past year, the assessment of the individual’s capacity to fulfil their occupational responsibilities from a health perspective in two years, and assessment of mental health utilized in the workplace over the past three months.
In the present study, the overall WAI score was calculated according to the standard scoring procedure and used as a global indicator of work ability. The seven individual dimensions were not analyzed separately. This approach has been adopted in numerous previous studies and allows for an integrated assessment of functional capacity, health status, and perceived ability to meet job demands [23].
The WAI is a self-reported instrument and does not provide clinical diagnoses. Several of its components are directly related to health status, including diagnosed diseases, work impairment due to illness, sickness absence, and expectations regarding future work ability. As a result, the WAI represents a multidimensional construct that combines health-related factors with perceived work performance. In the present study, work ability was therefore conceptualized as an overall indicator reflecting both health and functional capacity, rather than being interpreted as a purely medical or purely performance-based outcome. The potential conceptual overlap between work ability and general health was taken into account in the interpretation of the findings.
Conceptual model and statistical analysis
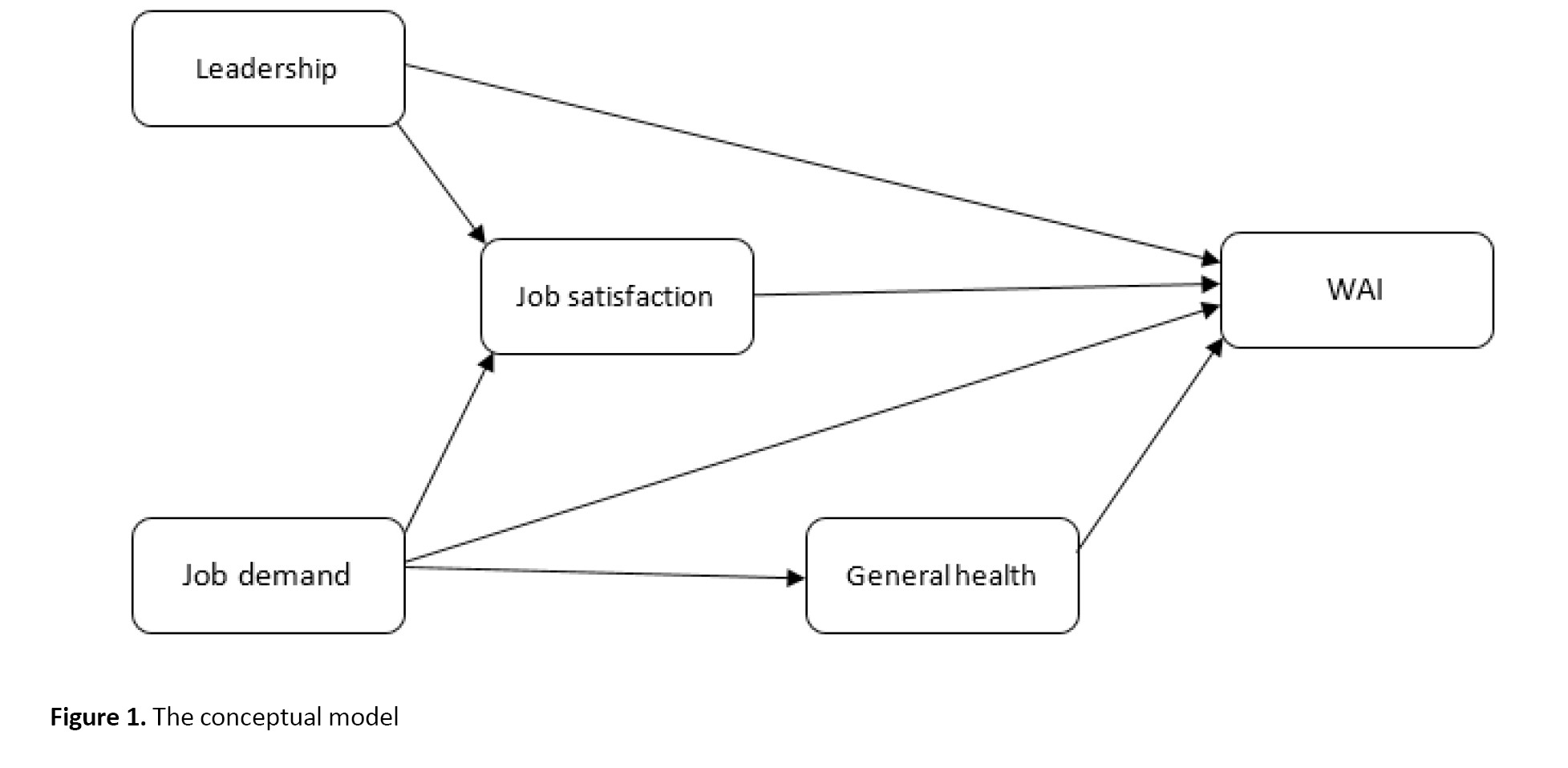
A conceptual model based on the JD-R framework was developed to examine relationships among study variables (Figure 1).
Work ability (WA) was initially conceived in the 1980s by the Finnish Institute of Occupational Health to evaluate workplace health and age-related work capacity [1]. It reflects the balance between individual resources and job demands, encompassing physical and mental capacities, work characteristics, and future ability to meet job requirements [2].
WA is a multifactorial construct influenced by numerous individual and occupational factors. Prior reviews have identified a wide variety of antecedents, including physical, mental, emotional, and psychosocial job demands; work conditions; job resources; job control; fairness; and job security, as well as demographic characteristics, health status, and lifestyle factors [3-5].
Although initial efforts have been made to examine factors influencing WA, the mechanisms through which organizational and psychosocial variables jointly shape WA remain insufficiently understood. Most prior studies have investigated these factors separately, limiting the development of integrated explanatory models [5].
Theoretical frameworks such as lifespan development [6], job demand-resources [7], and job demand-control [8] provide useful foundations for understanding WA, proposing that job demands contribute to health impairment while job resources, including supportive leadership, enhance motivation and work ability [9]. The job demands-resources (JD-R) model stands out as a particularly comprehensive and flexible framework [8]. However, existing empirical research rarely incorporates these theoretical elements into a single comprehensive structural equation model that captures the direct and indirect interactions among job demands, leadership, job satisfaction, and general health [3].
Healthcare workers face high emotional labor, role ambiguity, heavy workload, and continuous exposure to human suffering, all of which may influence WA. Numerous studies have examined the association between WA and physical/mental/psychosocial job demands [10-12]. However, these findings are mixed, likely due to differences in job contexts, variations in how job demands are defined, and the influence of moderating organizational factors [13]. Leadership and job satisfaction have also been identified as relevant psychosocial variables, with evidence suggesting that effective leadership enhances job satisfaction and may indirectly support WA [14, 15]. Nevertheless, the mediating roles of job satisfaction and general health remain theoretically underdeveloped and empirically under examined within comprehensive structural equation models based on the JD-R framework [16].
Given these limitations, there is a clear need for integrated models that simultaneously assess organizational, psychosocial, and individual variables to clarify their combined direct and indirect effects on WA. Such comprehensive analyses are particularly scarce in non-Western settings and among healthcare workers. Therefore, the present study develops and tests a comprehensive structural equation model fully grounded in the JD-R model. This study aimed to explore and test the pathways between psychosocial factors and work ability among Iranian healthcare workers. Data were analyzed using structural equation modeling (SEM) to examine the direct and indirect effects of psychosocial factors, including job demands, leadership, job satisfaction, and general health. The study focused on psychosocial factors within the JD-R framework rather than a comprehensive structural model.
Materials and Methods
The participants in this cross-sectional study were employees of township healthcare centers in northern Iran. A stratified random sampling method was used to ensure representativeness across different healthcare units. Stratification was based on the type of healthcare unit (clinics, hospitals, and rural and urban healthcare centers) to ensure proportional representation from each unit. Within each stratum, the participants were randomly selected from the list of eligible healthcare professionals, including nurses, physicians, midwives, and allied health staff. The number of participants in each stratum was determined proportionally to the size of the unit to maintain representativeness.
The inclusion criteria were clearly defined as healthcare practitioners directly engaged in patient care or healthcare delivery, including nurses, physicians, midwives, and allied health staff, with at least 1 year of work experience. The exclusion criteria comprised administrative personnel, office staff, accountants, cleaning workers, and others not directly engaged in healthcare provision. As the health centers include various medical and health departments (healthcare clinics, hospitals, and rural and urban healthcare centers), only eligible healthcare workers meeting these criteria were included. Out of 579 invited participants, 579 completed the questionnaire and were included in the analysis (response rate: 100%). Non-response bias was therefore not applicable. All participants met the inclusion criteria of becoming healthcare practitioners intimately engaged in patient care or healthcare service delivery. A self-administered questionnaire was used to gather data on demographic and job-related characteristics (age, job experience, job type, and gender) and study variables. Before data collection, the study objectives were clearly explained, and Informed consent was acquired from all individuals.
Psychosocial factors and general health
To assess job demands, leadership status, job satisfaction, and general health, items from the second version of the Copenhagen psychosocial questionnaire (COPSOQ II) were used. The COPSOQ II, as a multi-theory-based instrument, is appropriate for a wide range of analytical levels. The psychometric properties of the COPSOQ have been validated across multiple languages [17]. We used selected subscales from COPSOQ II, specifically the emotional job demand dimension and items reflecting quantitative workload, to focus on the most relevant aspects of job demands affecting healthcare workers in this context [18]. Although the official, validated Persian version does not include a formal “quantitative demands” dimension, these items were adapted from prior literature and contextualized to reflect the most significant workload intensity and emotional challenges faced by healthcare professionals [19].
Other dimensions of COPSOQ II were not included to reduce participant burden and because they were deemed less critical for the current study’s aims. The reliability of the Persian version was verified, with a Cronbach α ranging from 0.75 to 0.89 [20]. Some items included “How often do you not have time to complete all your work tasks?”, “Is your work unevenly distributed so it piles up?”, and “Is your work emotionally demanding?” A 5-option scoring system was used to rate responses (1=always; 2=often; 3=sometimes; 4=seldom; 5=never or hardly ever). Leadership quality was assessed using 4 items, with each person directly evaluating their manager. The items included “Makes sure that the individual member of staff has good development opportunities,” “Gives high priority to job satisfaction,” “Is good at work planning?”, and “Is good at solving conflicts?” The items were rated on a 5-point Likert scale ranging from 1 (to a very small extent) to 5 (to a very large extent). Job satisfaction was measured by considering participants’ perspectives on future job prospects, the physical condition of the work environment, and the use of their skills. Participants rated their satisfaction on a scale from “very dissatisfied” to “very satisfied.”
Furthermore, a single-item scale was used to assess general health, in which participants rated their overall health. The response options ranged from “excellent=1” to “poor=5.” We acknowledge that using a single-item measure may limit psychometric robustness for latent variable modeling. However, evidence from prior studies indicates that single-item measures of health can serve as valid and reliable proxies for general health in epidemiological and occupational health research [21], and limitations are discussed in the manuscript.
Work ability
Despite the availability of numerous instruments to assess work ability, the work ability index (WAI) has been employed more extensively. The WAI is the product of a multidisciplinary team encompassing psychology, physiology, medicine, biostatistics, and epidemiology [22]. The WAI comprises 60 items organized into 7 dimensions: current WA relative to a lifetime best, WA in relation to the demands of the job, amount of physician-diagnosed diseases (indicated by the participant on a checklist of 50 potential diseases), evaluation of impairment resulting from disease or injury, total sick leave days accrued in the past year, the assessment of the individual’s capacity to fulfil their occupational responsibilities from a health perspective in two years, and assessment of mental health utilized in the workplace over the past three months.
In the present study, the overall WAI score was calculated according to the standard scoring procedure and used as a global indicator of work ability. The seven individual dimensions were not analyzed separately. This approach has been adopted in numerous previous studies and allows for an integrated assessment of functional capacity, health status, and perceived ability to meet job demands [23].
The WAI is a self-reported instrument and does not provide clinical diagnoses. Several of its components are directly related to health status, including diagnosed diseases, work impairment due to illness, sickness absence, and expectations regarding future work ability. As a result, the WAI represents a multidimensional construct that combines health-related factors with perceived work performance. In the present study, work ability was therefore conceptualized as an overall indicator reflecting both health and functional capacity, rather than being interpreted as a purely medical or purely performance-based outcome. The potential conceptual overlap between work ability and general health was taken into account in the interpretation of the findings.
Conceptual model and statistical analysis
A conceptual model based on the JD-R framework was developed to examine relationships among study variables (Figure 1).
The model was specified using SEM to estimate simultaneous direct and indirect paths among the variables, guided by the JD-R framework. Leadership was hypothesized to be positively associated with job satisfaction (β=0.47) and to have a potential direct effect on work ability. In contrast, job demands were expected to negatively affect work ability, general health, and job satisfaction (β=-0.19). General health and job satisfaction were initially considered as potential mediators to explore indirect pathways between psychosocial factors and work ability. Model paths were constructed a priori and informed by previous literature [15, 16, 24, 25]. Descriptive statistics summarized sociodemographic characteristics and study variables. The Pearson correlation was used to examine associations between psychosocial factors and work ability. SEM with maximum-likelihood estimation was then applied to test the hypothesized relationships. Model assumptions, including normality, linearity, and the absence of multicollinearity, were checked and found to be satisfied. Goodness-of-fit indices included root mean square error of approximation (RMSEA)<0.08, goodness of fit index (GFI) >0.8, comparative fit index (CFI) >0.9, and Tucker-Lewis index (TLI) >0.9 [26].
Minor post-hoc modifications based on modification indices were made to improve model fit, including the removal of the non-significant direct path from general health to work ability and the addition of a path from job demands to job satisfaction. These modifications were theoretically justified and did not alter the core hypothesized structure of the JD-R model.
Results
A total of 579 healthcare workers participated in the study, all of whom completed the questionnaires, resulting in a response rate of 100%. The majority of participants were female (60.1%), with a Mean±SD age of 36.2±8.5 years (range: 22–65 years). The mean job experience was 11.3±8 years (range: 1–31 years). All employees worked full-time, with most following a standard one-shift schedule. Additionally, 65.6% of participants held at least a bachelor’s degree.
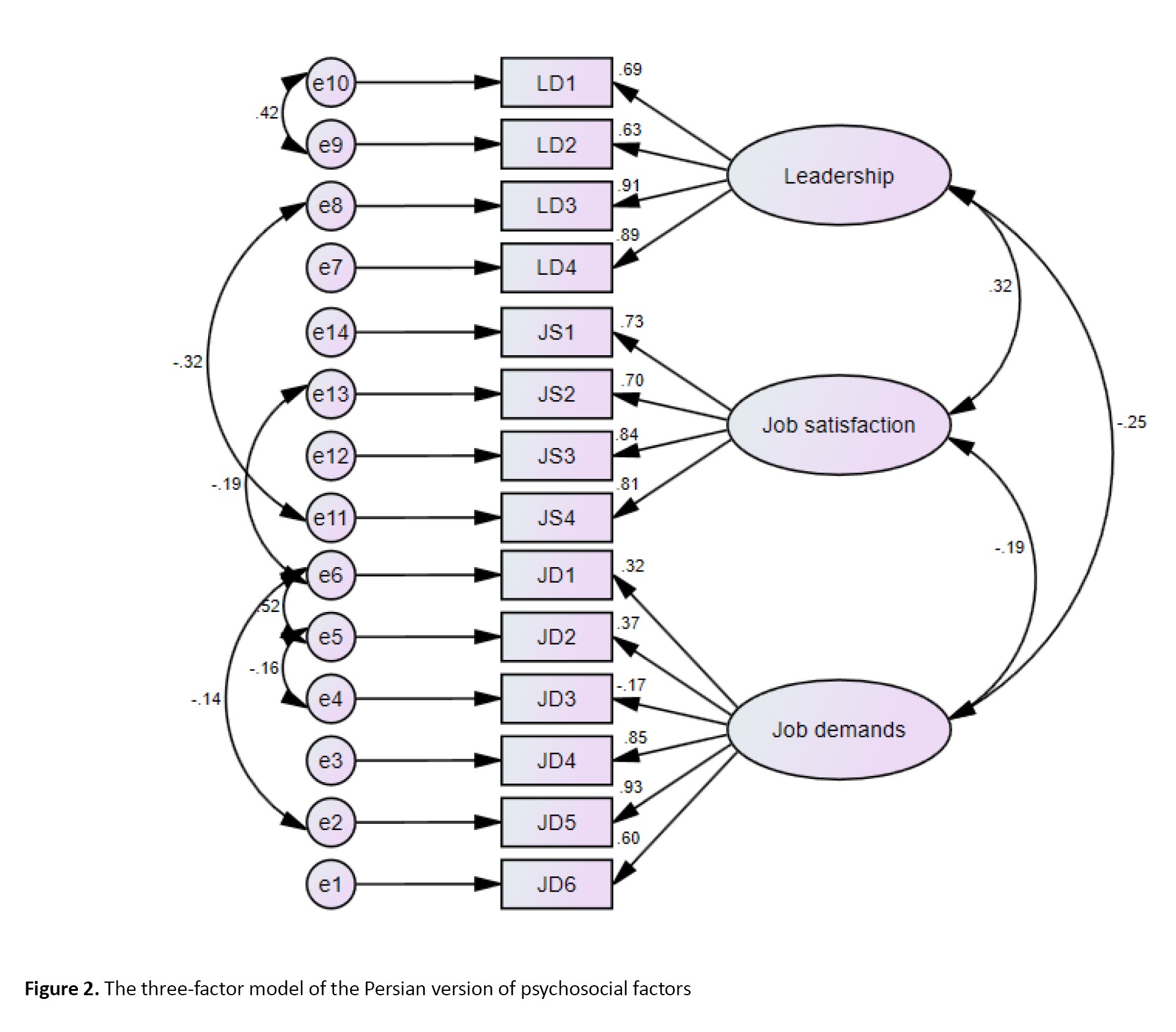
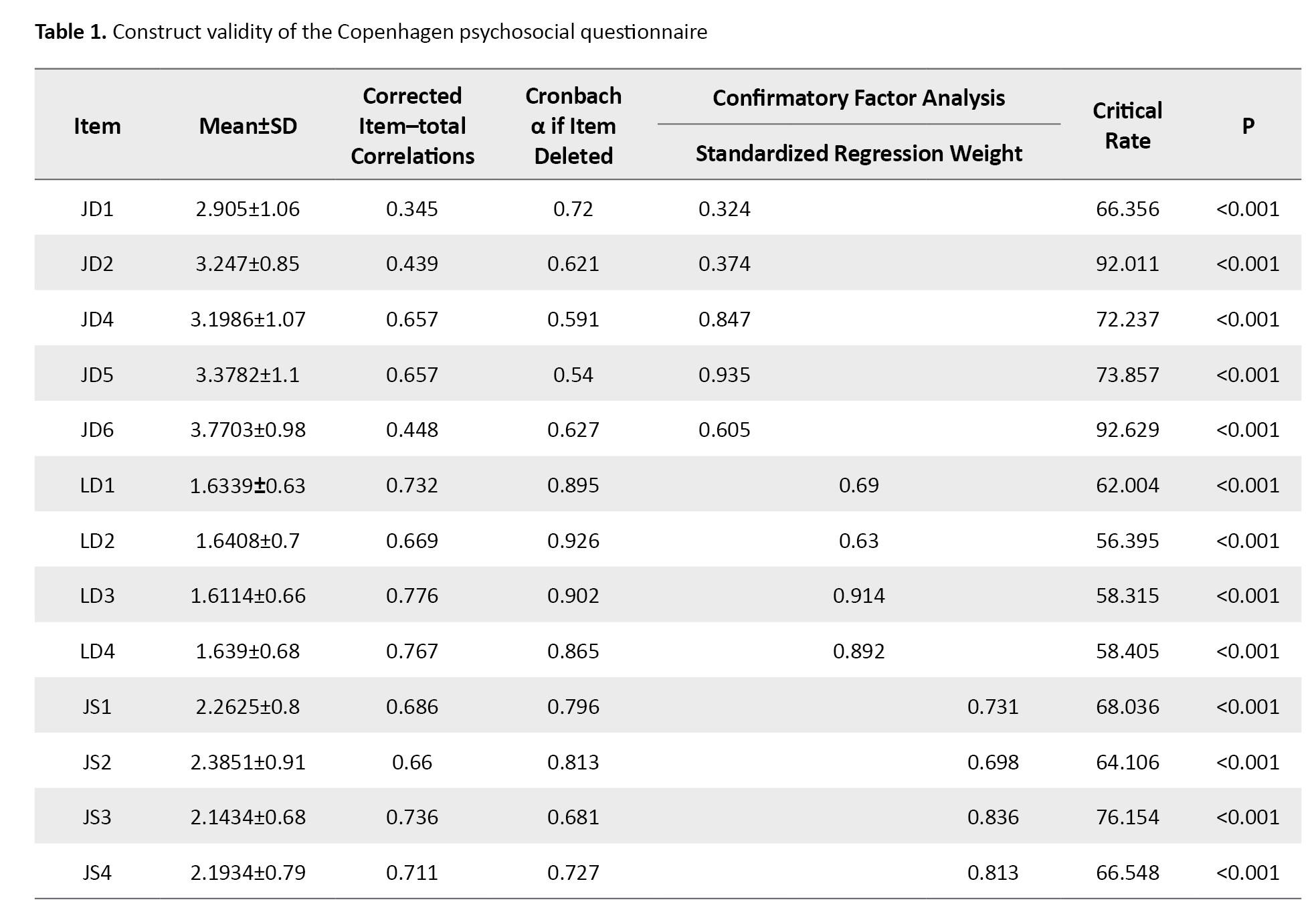
The questionnaire used to measure the study variables was developed based on a comprehensive literature review and expert panel input to ensure content validity and relevance. Construct validity was assessed using confirmatory factor analysis (CFA), and internal consistency was evaluated using the Cronbach α. The psychometric results confirmed the instrument’s validity and reliability within this sample. The average Cronbach’s α values for job demands, leadership, and job satisfaction were 0.71, 0.92, and 0.81, respectively (Table 1).
The fit of the structural model was evaluated using various goodness-of-fit metrics (Table 2).
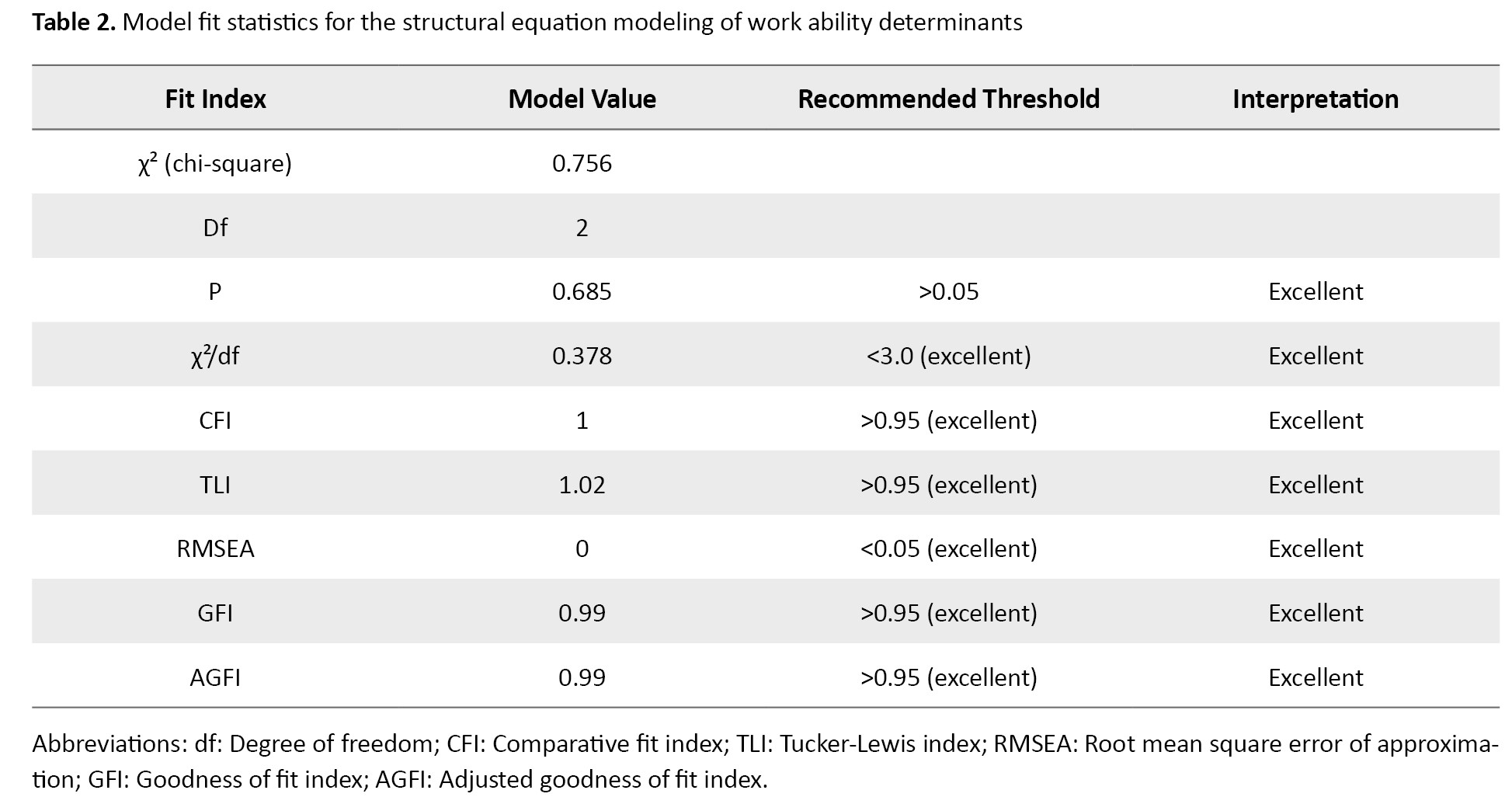
The initial model demonstrated excellent fit across all indices: χ²=0.756 (df=2, P=0.685), χ²/df=0.378, CFI=1, TLI=1.02, GFI=0.99, adjusted GFI=0.99, and RMSEA=0. These values indicate an excellent fit between the model and the observed data. Figure 2 displays the paths and factor loadings for the study scales and items.
Minor post-hoc modifications based on modification indices were made to improve model fit, including the removal of the non-significant direct path from general health to work ability and the addition of a path from job demands to job satisfaction. These modifications were theoretically justified and did not alter the core hypothesized structure of the JD-R model.
Results
A total of 579 healthcare workers participated in the study, all of whom completed the questionnaires, resulting in a response rate of 100%. The majority of participants were female (60.1%), with a Mean±SD age of 36.2±8.5 years (range: 22–65 years). The mean job experience was 11.3±8 years (range: 1–31 years). All employees worked full-time, with most following a standard one-shift schedule. Additionally, 65.6% of participants held at least a bachelor’s degree.
The questionnaire used to measure the study variables was developed based on a comprehensive literature review and expert panel input to ensure content validity and relevance. Construct validity was assessed using confirmatory factor analysis (CFA), and internal consistency was evaluated using the Cronbach α. The psychometric results confirmed the instrument’s validity and reliability within this sample. The average Cronbach’s α values for job demands, leadership, and job satisfaction were 0.71, 0.92, and 0.81, respectively (Table 1).
The fit of the structural model was evaluated using various goodness-of-fit metrics (Table 2).
The initial model demonstrated excellent fit across all indices: χ²=0.756 (df=2, P=0.685), χ²/df=0.378, CFI=1, TLI=1.02, GFI=0.99, adjusted GFI=0.99, and RMSEA=0. These values indicate an excellent fit between the model and the observed data. Figure 2 displays the paths and factor loadings for the study scales and items.
Table 3 provides descriptive statistics and correlations among the study variables.
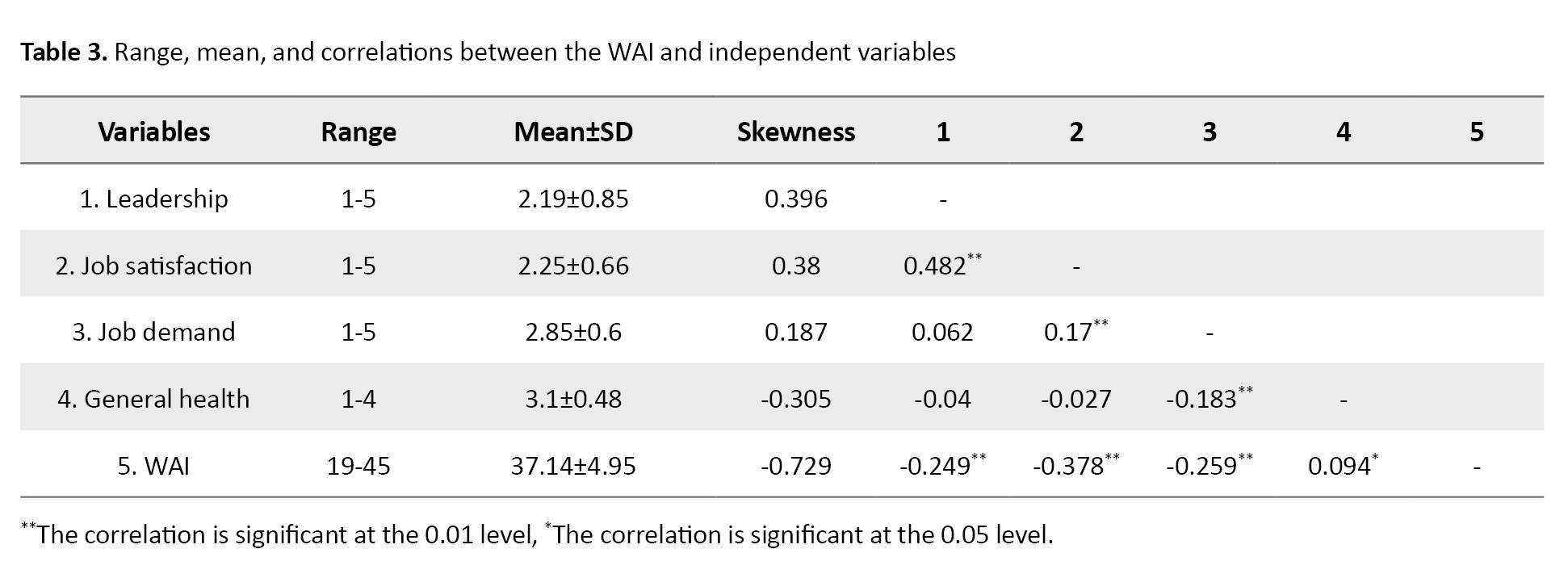
The WAI was significantly negatively correlated with leadership (r=-0.249, P<0.01), job satisfaction (r=-0.378, P<0.01), and job demand (r=-0.259, P<0.01). At the same time, a weaker positive correlation was observed with general health (r=0.094, P<0.05). These correlation directions were unexpected and should be considered exploratory findings. The structural equation model revealed a negative direct effect of job demands on WAI (β=−0.19), reflecting their unique contribution after accounting for mediating variables such as job satisfaction. The weak and non-significant effect of general health suggests its mediating role is limited.
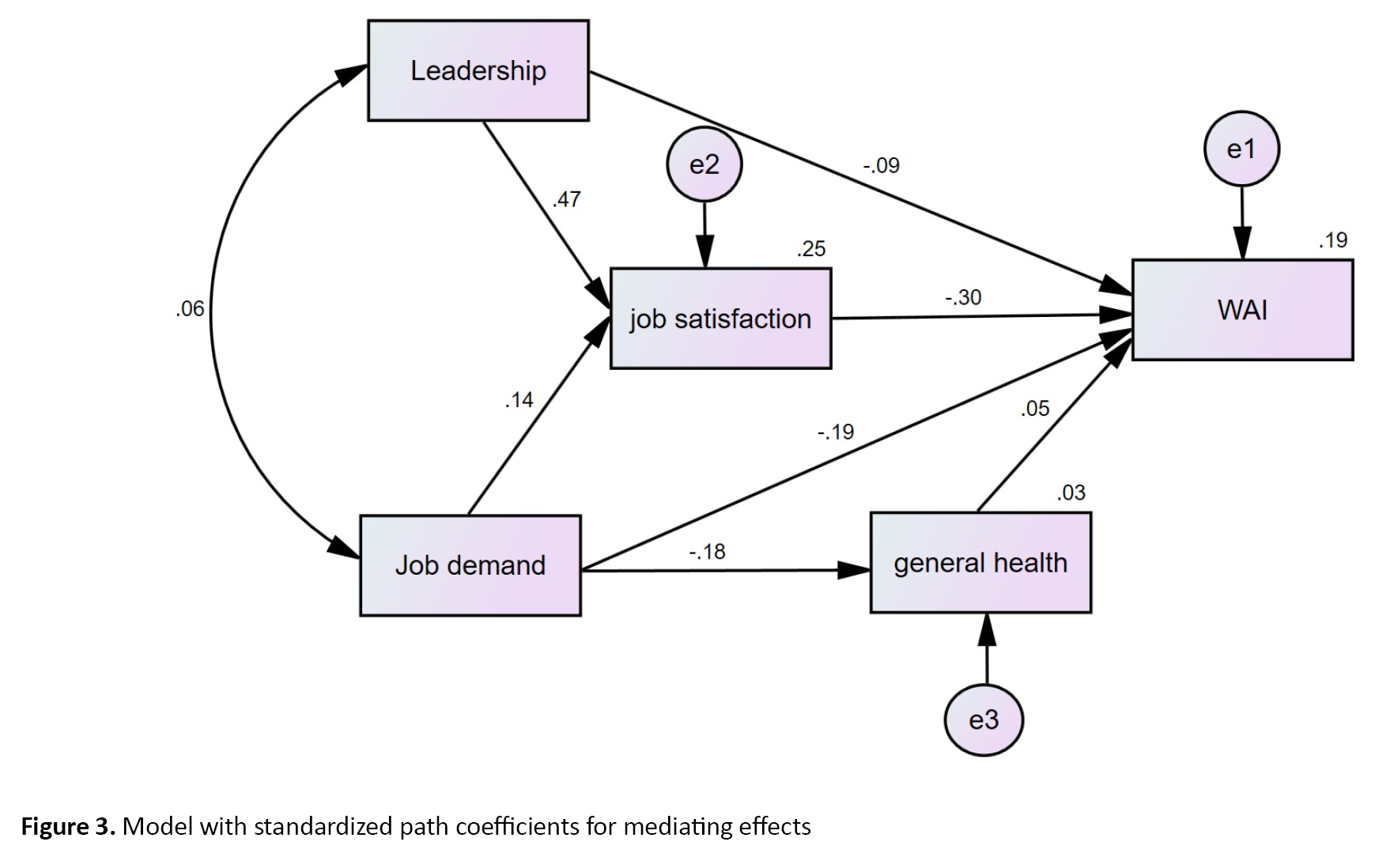
Following AMOS guidelines, several model modifications were made. Specifically, the non-significant direct path from general health to work ability was removed, and a path from job demands to job satisfaction was added to improve model fit (Figure 3).
The WAI was significantly negatively correlated with leadership (r=-0.249, P<0.01), job satisfaction (r=-0.378, P<0.01), and job demand (r=-0.259, P<0.01). At the same time, a weaker positive correlation was observed with general health (r=0.094, P<0.05). These correlation directions were unexpected and should be considered exploratory findings. The structural equation model revealed a negative direct effect of job demands on WAI (β=−0.19), reflecting their unique contribution after accounting for mediating variables such as job satisfaction. The weak and non-significant effect of general health suggests its mediating role is limited.
Following AMOS guidelines, several model modifications were made. Specifically, the non-significant direct path from general health to work ability was removed, and a path from job demands to job satisfaction was added to improve model fit (Figure 3).
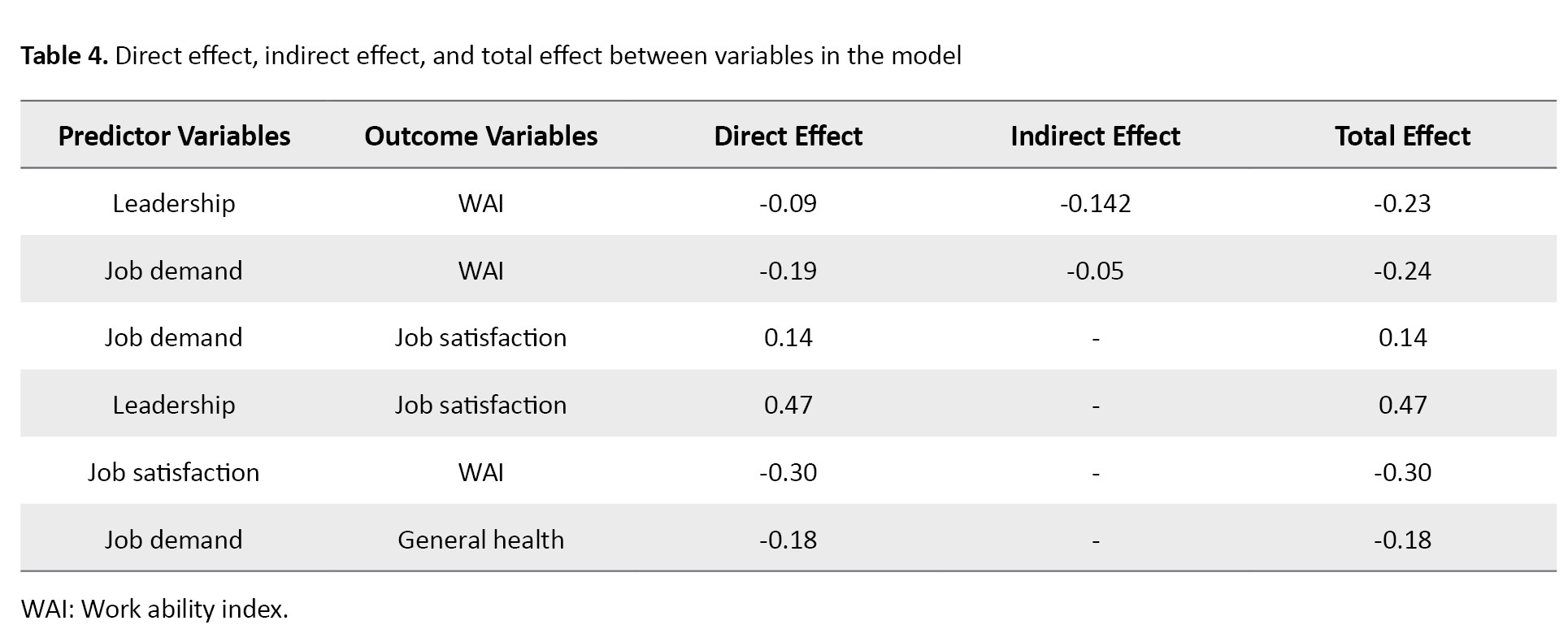
In the finalized model, leadership had a significant positive direct effect on job satisfaction (β=0.47, P<0.001), while job demands negatively predicted work ability (β=-0.19, P<0.001). Leadership had a negative indirect effect on work ability through job satisfaction (β=-0.142), yielding a total effect of −0.23. Job demands also had a positive direct effect on job satisfaction (β=0.14, P<0.001) and a minor negative effect on general health (β=−0.18, P<0.001). Job satisfaction itself negatively affected work ability (β=−0.30, P<0.001). The direct, indirect, and total effects are summarized in Table 4.
Discussion
This study examined the relationships among job satisfaction, job demands, leadership, general health, and work ability using structural equation modeling (SEM) within the JD-R framework, highlighting the direct and indirect pathways through which psychosocial factors may influence work ability among healthcare workers. The focus remained on psychosocial factors, rather than a comprehensive structural model with multiple latent constructs.
Job satisfaction showed a significant negative association with WAI and had a direct negative effect in the structural model. This finding indicates that poorer job satisfaction is associated with reduced work ability. In demanding healthcare environments, low job satisfaction may reflect increased job strain, emotional exhaustion, unmet expectations, and chronic job stress, which are recognized contributors to diminished work ability [22, 27].
A weak association was observed between self-rated general health and work ability, consistent with previous evidence indicating that work ability is associated with physical and mental health [28]. However, the direct path between general health and work ability was not statistically significant in the SEM. This finding may reflect the dominant influence of psychosocial work-related factors, such as job demands and job satisfaction, on how perceived health status translates into work performance [29]. In addition, the use of self-reported measures of general health may not fully capture its multidimensional nature, as objective clinical indicators often show stronger associations with work ability than subjective health assessments [30]. Despite the non-significant direct effect, general health was retained in the model due to its strong theoretical relevance within occupational health frameworks, including the JD-R model. Similar inconsistencies have been reported in previous studies when psychosocial variables are simultaneously considered [25]. Moreover, failure to distinguish between perceived and objective dimensions of work ability may obscure the relationship between health status and work performance [3].
The SEM results validated both direct and indirect pathways among job demands, leadership, job satisfaction, and work ability. Job demands had a negative direct effect on work ability, whereas leadership influenced work ability indirectly through job satisfaction. These findings are consistent with previous studies using structural models to examine similar relationships [24, 25, 31].
Leadership played an important indirect role by shaping job satisfaction, which in turn affected work ability. Poorer leadership quality was associated with lower job satisfaction, leading to reduced work ability. This pattern is consistent with the Path–Goal theory, which emphasizes leadership as a motivational and supportive resource rather than a direct determinant of performance outcomes [32]. Poor leadership quality may impair work ability to a degree comparable to high job demands or unfavorable working conditions [22].
The strong negative direct effect of job demands on work ability observed in this study supports the JD-R model and life development theory, which emphasize the detrimental impact of excessive demands on individual capacity over time [33].
Conclusion
This study explored the direct and indirect relationships among job demands, leadership, job satisfaction, general health, and work ability within the JD-R framework among Iranian healthcare workers. Contrary to theoretical expectations, leadership showed a negative total effect on work ability through job satisfaction, while job demands negatively influenced work ability directly and indirectly. Job satisfaction was negatively associated with work ability, and general health showed a weak, non-significant effect in the final model. These findings highlight that, in this sample, higher perceived leadership quality and job satisfaction did not translate into increased work ability, suggesting that contextual or cultural factors may influence these associations. Overall, the results underscore the complex interplay of psychosocial factors in determining work ability and indicate the need for further research to clarify unexpected relationships and guide interventions to optimize work ability among healthcare professionals.
Study limitations
This study possesses various limitations that must be acknowledged when evaluating the results. The cross-sectional approach limits the ability to infer causal links among the examined variables. Second, the study’s scope was limited by the number of observed variables and the degrees of freedom (df) in the structural model, which were remarkably low (df=2) when corrections based on fit indices were applied. This low df may inflate results, and therefore, findings should be interpreted with caution. Third, some constructs, such as overall work ability (WAI) and job satisfaction, were measured with a limited number of items, potentially reducing the model’s power and increasing the risk of conflicting coefficients. Fourth, the use of the partial COPSOQ model may not fully capture all dimensions of psychosocial factors at work. Finally, although statistical analyses were conducted to compare with previous research, the model’s generalizability to other organizational or cultural contexts warrants further exploration in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1400.615). All participants were informed of the study’s objectives and provided written informed consent before participation.
Funding
The paper was extracted from the master's thesis of Azimeh Kalteh, approved by the Department of Occupational Health Engineering, Faculty of Health, Mazandaran University of Medical Sciences, Sari, Iran.
Authors contributions
Conceptualization, supervision, funding acquisition and resources: Hajiomid Kalteh and Siavash Etemadinezhad; Methodology: Hajiomid Kalteh, Siavash Etemadinezhad, and Solale Ramzani; Data collection: Solale Ramzani and Azimeh Kalteh; Data analysis: Soudabeh HamediShahraki and Seyed-Nouraddin Mousavinasab; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to express their sincere gratitude to the healthcare workers who participated in this study for their valuable time and contributions. We also appreciate the support provided by Mazandaran University of Medical Sciences—special thanks to the experts who reviewed the questionnaire and contributed to improving its validity.
Discussion
This study examined the relationships among job satisfaction, job demands, leadership, general health, and work ability using structural equation modeling (SEM) within the JD-R framework, highlighting the direct and indirect pathways through which psychosocial factors may influence work ability among healthcare workers. The focus remained on psychosocial factors, rather than a comprehensive structural model with multiple latent constructs.
Job satisfaction showed a significant negative association with WAI and had a direct negative effect in the structural model. This finding indicates that poorer job satisfaction is associated with reduced work ability. In demanding healthcare environments, low job satisfaction may reflect increased job strain, emotional exhaustion, unmet expectations, and chronic job stress, which are recognized contributors to diminished work ability [22, 27].
A weak association was observed between self-rated general health and work ability, consistent with previous evidence indicating that work ability is associated with physical and mental health [28]. However, the direct path between general health and work ability was not statistically significant in the SEM. This finding may reflect the dominant influence of psychosocial work-related factors, such as job demands and job satisfaction, on how perceived health status translates into work performance [29]. In addition, the use of self-reported measures of general health may not fully capture its multidimensional nature, as objective clinical indicators often show stronger associations with work ability than subjective health assessments [30]. Despite the non-significant direct effect, general health was retained in the model due to its strong theoretical relevance within occupational health frameworks, including the JD-R model. Similar inconsistencies have been reported in previous studies when psychosocial variables are simultaneously considered [25]. Moreover, failure to distinguish between perceived and objective dimensions of work ability may obscure the relationship between health status and work performance [3].
The SEM results validated both direct and indirect pathways among job demands, leadership, job satisfaction, and work ability. Job demands had a negative direct effect on work ability, whereas leadership influenced work ability indirectly through job satisfaction. These findings are consistent with previous studies using structural models to examine similar relationships [24, 25, 31].
Leadership played an important indirect role by shaping job satisfaction, which in turn affected work ability. Poorer leadership quality was associated with lower job satisfaction, leading to reduced work ability. This pattern is consistent with the Path–Goal theory, which emphasizes leadership as a motivational and supportive resource rather than a direct determinant of performance outcomes [32]. Poor leadership quality may impair work ability to a degree comparable to high job demands or unfavorable working conditions [22].
The strong negative direct effect of job demands on work ability observed in this study supports the JD-R model and life development theory, which emphasize the detrimental impact of excessive demands on individual capacity over time [33].
Conclusion
This study explored the direct and indirect relationships among job demands, leadership, job satisfaction, general health, and work ability within the JD-R framework among Iranian healthcare workers. Contrary to theoretical expectations, leadership showed a negative total effect on work ability through job satisfaction, while job demands negatively influenced work ability directly and indirectly. Job satisfaction was negatively associated with work ability, and general health showed a weak, non-significant effect in the final model. These findings highlight that, in this sample, higher perceived leadership quality and job satisfaction did not translate into increased work ability, suggesting that contextual or cultural factors may influence these associations. Overall, the results underscore the complex interplay of psychosocial factors in determining work ability and indicate the need for further research to clarify unexpected relationships and guide interventions to optimize work ability among healthcare professionals.
Study limitations
This study possesses various limitations that must be acknowledged when evaluating the results. The cross-sectional approach limits the ability to infer causal links among the examined variables. Second, the study’s scope was limited by the number of observed variables and the degrees of freedom (df) in the structural model, which were remarkably low (df=2) when corrections based on fit indices were applied. This low df may inflate results, and therefore, findings should be interpreted with caution. Third, some constructs, such as overall work ability (WAI) and job satisfaction, were measured with a limited number of items, potentially reducing the model’s power and increasing the risk of conflicting coefficients. Fourth, the use of the partial COPSOQ model may not fully capture all dimensions of psychosocial factors at work. Finally, although statistical analyses were conducted to compare with previous research, the model’s generalizability to other organizational or cultural contexts warrants further exploration in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1400.615). All participants were informed of the study’s objectives and provided written informed consent before participation.
Funding
The paper was extracted from the master's thesis of Azimeh Kalteh, approved by the Department of Occupational Health Engineering, Faculty of Health, Mazandaran University of Medical Sciences, Sari, Iran.
Authors contributions
Conceptualization, supervision, funding acquisition and resources: Hajiomid Kalteh and Siavash Etemadinezhad; Methodology: Hajiomid Kalteh, Siavash Etemadinezhad, and Solale Ramzani; Data collection: Solale Ramzani and Azimeh Kalteh; Data analysis: Soudabeh HamediShahraki and Seyed-Nouraddin Mousavinasab; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to express their sincere gratitude to the healthcare workers who participated in this study for their valuable time and contributions. We also appreciate the support provided by Mazandaran University of Medical Sciences—special thanks to the experts who reviewed the questionnaire and contributed to improving its validity.
References
- Ebener M, Hasselhorn HM. Validation of short measures of work ability for research and employee surveys. International Journal of Environmental Research and Public Health. 2019; 16(18):3386. [DOI:10.3390/ijerph16183386] [PMID]
- Garthe N, Hasselhorn HM. The relationship between voluntary employer change and work ability among older workers: Investigating the honeymoon-hangover effect. Journal for Labour Market Research. 2021; 55(1):12. [DOI:10.1186/s12651-021-00294-0]
- Cadiz DM, Brady G, Rineer JR, Truxillo DM. A review and synthesis of the work ability literature. Work, Aging and Retirement. 2019; 5(1):114-38. [DOI:10.1093/workar/way010]
- Mokarami H, Kalteh HO, Marioryad H. The effect of work-related and sociodemographic factors on work ability index (WAI) among Iranian workers. Work. 2020; 65(1):137-43. [DOI:10.3233/WOR-193066] [PMID]
- Hlaďo P, Pokorný B, Petrovová M. Work ability of the Czech workforce aged 50+ and the relationship between selected demographic and anthropometric variables. Kontakt. 2017; 19(2):e145-55. [DOI:10.1016/j.kontakt.2017.05.001]
- Greve W. Adaptation across the lifespan: Towards a processual evolutionary explanation of human development. Integrative Psychological and Behavioral Science. 2023; 57(4):1119-39. [DOI:10.1007/s12124-023-09767-y] [PMID]
- Kulikowski K, Orzechowski J. All employees need job resources: Testing the job demands-resources theory among employees with either high or low working memory and fluid intelligence. Medycyna Pracy. 2018; 69(5):483-96. [DOI:10.13075/mp.5893.00709] [PMID]
- Bakker AB, Demerouti E. Job demands-resources theory: Taking stock and looking forward. Journal of Occupational Health Psychology. 2017; 22(3):273-85. [DOI:10.1037/ocp0000056] [PMID]
- Li Y, Chen C, Yuan Y. Evolving the job demands-resources framework to JD-R 3.0: The impact of after-hours connectivity and organizational support on employee psychological distress. Acta Psychologica. 2025; 253:104710. [DOI:10.1016/j.actpsy.2025.104710] [PMID]
- Habibi E, Dehghan H, Zeinodini M, Yousefi H, Hasanzadeh A. A study on work ability index and physical work capacity based on the VO₂max fax equation in male nursing hospital staff in Isfahan, Iran. International Journal of Preventive Medicine. 2012; 3(11):776-80. [PMID]
- Riedel N, Müller A, Ebener M. Applying strategies of selection, optimization, and compensation to maintain work ability: A psychosocial resource complementing the job demand-control model. Journal of Occupational and Environmental Medicine. 2015; 57(5):552-61. [DOI:10.1097/JOM.0000000000000402] [PMID]
- Boelhouwer IG, Vermeer W, van Vuuren T. The associations between late effects of cancer treatment, work ability and job resources: A systematic review. International Archives of Occupational and Environmental Health. 2021; 94(2):147-89. [DOI:10.1007/s00420-020-01567-w] [PMID]
- Tims M, Bakker AB, Xanthopoulou D. Do transformational leaders enhance their followers' daily work engagement? The Leadership Quarterly. 2011; 22(1):121-31. [DOI:10.1016/j.leaqua.2010.12.011]
- Dongoran AP, Wibowo RP. Analysis of effect of leadership style, work motivation and work ability to employee satisfaction in increasing performance of harvesters. IOP Conference Series: Materials Science and Engineering. 2020; 801(1):1-11. [Link]
- Richter A, Roczniewska M, Loeb C, Stempel CR, Rigotti T. The cross-level moderation effect of resource-providing leadership on the demands-work ability relationship. International Journal of Environmental Research and Public Health. 2021; 18(17):9084. [DOI:10.3390/ijerph18179084] [PMID]
- Airila A, Hakanen JJ, Schaufeli WB, Luukkonen R, Punakallio A, Lusa S. Are job and personal resources associated with work ability 10 years later? The mediating role of work engagement. Work and Stress. 2014; 28(1):87-105. [DOI:10.1080/02678373.2013.872208]
- Etemadinezhad S, Kalteh HO, Mousavinasab SN, Mohsenabadi M. Psychometric properties of the Persian version of the Copenhagen Psychosocial Questionnaire (COPSOQ III). Journal of Occupational Health and Epidemiology. 2023; 12(3):163-74. [DOI:10.61186/johe.12.3.163]
- Burr H, Berthelsen H, Moncada S, Nübling M, Dupret E, Demiral Y, et al. The third version of the Copenhagen psychosocial questionnaire. Safety and Health at Work. 2019; 10(4):482-503. [DOI:10.1016/j.shaw.2019.10.002] [PMID]
- Berthelsen H, Hakanen JJ, Westerlund H. Copenhagen psychosocial questionnaire: A validation study using the job demand-resources model. PLoS One. 2018; 13(4):e0196450. [DOI:10.1371/journal.pone.0196450] [PMID]
- Aminian M, Dianat I, Miri A, Asghari-Jafarabadi M. The Iranian version of the Copenhagen psychosocial questionnaire (COPSOQ) for assessment of psychological risk factors at work. Health Promotion Perspectives. 2017; 7(1):7-13. [DOI:10.15171/hpp.2017.03] [PMID]
- Smith AB, Ware JE Jr, Aluko P, Kulasekaran A. The validity of single-item measures of health-related quality of life across groups differing in acute respiratory symptom severity. Quality of Life Research. 2024; 33(10):2773-80. [DOI:10.1007/s11136-024-03694-0] [PMID]
- Magnavita N, Meraglia I, Viti G, Borghese L. The work ability index (WAI) in the healthcare sector: A cross-sectional retrospective assessment. International Journal of Environmental Research and Public Health. 2024; 21(3):349. [DOI:10.3390/ijerph21030349] [PMID]
- Amirmahani M, Hasheminejad N, Tahernejad S, Nik HRT. Evaluation of work ability index and its association with job stress and musculoskeletal disorders among midwives during the COVID-19 pandemic. La Medicina del Lavoro. 2022; 113(4):e2022031. [DOI:10.23749/mdl.v113i4.12834] [PMID]
- Arshadi N, Zare R. Leadership effectiveness, perceived organizational support and work ability: Mediating role of job satisfaction. International Journal of Behavioral Sciences. 2016; 9(4):250-55. [Link]
- McGonagle AK, Fisher GG, Barnes-Farrell JL, Grosch JW. Individual and work factors related to perceived work ability and labor force outcomes. Journal of Applied Psychology. 2015; 100(2):376-98. [DOI:10.1037/a0037974] [PMID]
- Sathyanarayana S, Mohanasundaram T. Fit indices in structural equation modeling and confirmatory factor analysis: Reporting guidelines. Asian Journal of Economics, Business and Accounting. 2024; 24(7):561-77. [DOI:10.9734/ajeba/2024/v24i71430]
- Gharibi V, Mokarami H, Taban A, Aval MY, Samimi K, Salesi M. Effects of work-related stress on work ability index among Iranian workers. Safety and Health at Work. 2016; 7(1):43-8. [DOI:10.1016/j.shaw.2015.10.005] [PMID]
- Friedrich J, Rupp M, Feng YS, Sudeck G. Occupational health literacy and work ability: A moderation analysis including interpersonal and organizational factors in healthy organizations. Frontiers in Public Health. 2024; 12:1243138. [DOI:10.3389/fpubh.2024.1243138] [PMID]
- Zutautiene R, Kaliniene G, Ustinaviciene R, Radisauskas R. Prevalence of psychosocial work factors and stress and their associations with the physical and mental health of hospital physicians: A cross-sectional study in Lithuania. Frontiers in Public Health. 2023; 11:1123736. [DOI:10.3389/fpubh.2023.1123736] [PMID]
- Schaufeli WB, Taris TW. A critical review of the job demands-resources model: Implications for improving work and health. In: Bridging occupational, organizational and public health. Dordrech Springer; 2014. [DOI:10.1007/978-94-007-5640-3_4]
- Palermo J, Fuller-Tyszkiewicz M, Walker A, Appannah A. Primary- and secondary-level organizational predictors of work ability. Journal of Occupational Health Psychology. 2013; 18(2):220-30. [DOI:10.1037/a0031818] [PMID]
- Hussain MK, Khayat RAM. The impact of transformational leadership on job satisfaction and organisational commitment among hospital staff: A systematic review. Journal of Health Management. 2021; 23(4):614-30. [DOI:10.1177/09720634211050463]
- Ramzani S, Ghobadi K, Oveisi E, Hosseinnataj A, Samaei SE. Relationship between job satisfaction and various factors of the job demand-control-support model among Iranian nurses: Structural equation modeling study. Journal of Nursing and Midwifery Sciences. 2024; 11(4):e151314. [DOI:10.5812/jnms-151314]
Type of Study: Original Article |
Subject:
Occupational Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
