

Volume 14, Issue 1 (Winter 2026)
Iran J Health Sci 2026, 14(1): 57-64 |
Back to browse issues page


Ethics code: IR.QUMS.REC.1403.001
Clinical trials code: not Clinical trials
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
ebrahimi N, Pourrazi H, sadegi A. Breakfast Consumption and Its Association With Health, Cognitive, and Motor Functions in Girls Aged 7–11 Years. Iran J Health Sci 2026; 14 (1) :57-64
URL: http://jhs.mazums.ac.ir/article-1-1033-en.html
URL: http://jhs.mazums.ac.ir/article-1-1033-en.html



Department of Sport Sciences, Faculty of Social Sciences, Imam Khomeini International University, Qazvin, Iran. , pourrazi@soc.ikiu.ac.ir
Full-Text [PDF 646 kb]
(283 Downloads)
| Abstract (HTML) (665 Views)
References
Full-Text: (164 Views)
Introduction
Proper nutrition and adequate physical activity are fundamental determinants of optimal growth and health among school-aged children [1]. Recent global evidence indicates that unhealthy dietary behaviors and sedentary lifestyles contribute substantially to childhood overweight and obesity, which remain major public health challenges worldwide [2, 3]. Childhood and early school years represent a critical developmental window during which health-related behaviors are established and often track into adolescence and adulthood, thereby influencing long-term health outcomes [4, 5]. Childhood overweight and obesity are associated with adverse cardiometabolic consequences, including elevated blood pressure, dyslipidemia, and insulin resistance, many of which may persist into adulthood [6, 7]. While physical activity plays a crucial role in energy balance, dietary habits are equally important determinants of body weight and overall health status. Previous studies have shown that diet quality, independent of total energy intake, may significantly influence body weight and body mass index (BMI) in children [8]. Given the fundamental role of schools in children’s daily lives, school-based nutrition interventions, particularly those involving families, have been identified as effective strategies for promoting healthy eating behaviors and active lifestyles [8, 9]. Breakfast is commonly regarded as the first meal of the day and has been linked to several beneficial health and functional outcomes. Regular breakfast consumption has been associated with improved dietary quality, more favorable weight status, and better academic and cognitive performance among children and adolescents [10, 11].
Additionally, recent evidence suggests a positive association between breakfast consumption frequency and physical fitness indicators, such as cardiorespiratory endurance and muscular strength [12]. Nevertheless, findings across studies are not entirely consistent, and the mechanisms underlying these associations remain incompletely understood. Patterns of breakfast consumption vary across populations and are influenced by socioeconomic, cultural, and environmental factors. Studies conducted in different regions have reported a higher prevalence of breakfast skipping among girls, particularly those from lower socioeconomic backgrounds [11]. In Iran, several studies have examined breakfast consumption habits among school-aged children and adolescents, reporting considerable variability in consumption patterns and identifying factors such as time constraints, lack of appetite, and limited food availability as common reasons for breakfast omission [13, 14]. However, most Iranian studies have focused primarily on the prevalence of breakfast consumption or its association with obesity and academic performance, with limited attention to breakfast quality and functional outcomes. Moreover, there is a paucity of localized evidence examining the quantity and quality of breakfast consumption and their associations with anthropometric and functional outcomes among elementary school girls. In the present study, health indicators refer specifically to anthropometric measures commonly used to assess nutritional status and obesity-related health risks in children, including body weight, BMI, and waist-to-hip ratio (WHR). Therefore, this study aims to assess breakfast consumption status, including its frequency, quantity, and quality, and to investigate its association with selected physical health indicators as well as cognitive and motor function among girls aged 7–11 living in Qazvin, Iran. The findings of this study may provide valuable evidence for school administrators, public health practitioners, nutrition professionals, and policymakers to inform the development of targeted school-based nutrition programs and family-centered interventions to improve children’s health and functional outcomes.
Materials and Methods
This cross-sectional, descriptive–analytical correlational study was conducted among girl elementary school students studying in Qazvin, Iran, during the 2023–2024 academic year. The source population consisted of approximately 8000 girl students aged 7–11 years enrolled in public and private elementary schools.
The sample size was calculated using Cochran’s formula for correlation studies, assuming a confidence level of 95%, a statistical power of 80%, and an anticipated moderate correlation coefficient (r=0.15) based on previous similar studies. The minimum required sample size was estimated at 320 participants. To account for potential non-response and incomplete questionnaires, 365 students were initially recruited. A multistage cluster sampling method was employed. First, 2 educational districts in Qazvin were randomly selected as clusters. From each district, 1 public and 1 private elementary school were randomly chosen. Within each selected school, students were selected by simple random sampling using student identification numbers. Of the 365 recruited students, 45 were excluded due to incomplete questionnaires (n=31), withdrawal of consent (n=9), or absence during cognitive or motor testing sessions (n=5). Therefore, data from 320 participants were included in the final analysis, corresponding to a questionnaire non-completion rate of approximately 12.5%. No systematic differences were observed between included and excluded participants in terms of age or school type.
The inclusion criteria were girl students aged 7–11 years enrolled in elementary schools whose parents provided written informed consent. The exclusion criteria included any diagnosed chronic illness (e.g. diabetes, cardiovascular disease, and asthma), neurological or developmental disorders, use of medications affecting growth or cognitive function, adherence to medically prescribed dietary regimens, or unwillingness of the child or parent to participate.
Before the main study, a pilot study was conducted with 30 girl elementary school students from one school, which was not included in the final sample. The pilot aimed to assess the feasibility, clarity of questionnaire items, assessment duration, and logistical procedures. Based on feedback from parents and children, minor wording revisions were made to simplify questions related to breakfast quantity and food types, and the sequence of questionnaire sections was adjusted to improve comprehension.
Written informed consent was obtained from parents or legal guardians, and verbal assent was obtained from all participating children before data collection. Participation was voluntary, and confidentiality of all data was ensured. Body weight was measured twice using a calibrated Seca digital scale with participants barefoot and wearing light clothing; the mean value was recorded to the nearest 0.2 kg. Height was measured twice using a Seca stadiometer with participants standing upright, barefoot, heels together, and head positioned in the Frankfurt plane; the mean value was recorded to the nearest 0.5 cm. BMI was calculated as weight (kg)/height² (m²). Waist and hip circumferences were measured twice using a non-elastic tape in a standing position, and the mean values were used to calculate WHR.
Assessment methods for breakfast consumption status
Breakfast consumption was assessed using a researcher-developed questionnaire completed by students with parental assistance. The questionnaire consisted of 3 sections. The first section collected demographic and socioeconomic information, including age, parental education level, household income, and parental employment status. The second section assessed breakfast consumption patterns, including frequency, quantity, and types of foods consumed. The third section examined factors influencing breakfast consumption or omission among girls aged 7–11 years.
Breakfast consumption frequency was assessed using a 5-point Likert-type scale, reflecting the number of days breakfast was consumed at home during a typical week, with response options ranging from 0 days (no breakfast at home) to 4–5 days (regular breakfast at home). This variable was treated as an ordinal measure. Factors influencing breakfast consumption or non-consumption (including perceived health benefits of breakfast, liking breakfast, hunger, parental preparation, and parental pressure) were assessed using a similar 5-point Likert-type scale ranging from strongly disagree to agree strongly. No composite breakfast consumption score was calculated; therefore, each item was analyzed separately according to its measurement level.
Content validity of the questionnaire was established by an expert panel consisting of specialists in nutrition and public health. The content validity index (CVI) for the questionnaire was acceptable. Internal consistency reliability was assessed using the Cronbach α, yielding a coefficient of 0.81. Before the main study, the questionnaire was pilot-tested among 30 girl elementary school students from one school not included in the final sample to evaluate clarity, feasibility, and completion time. Based on feedback from the pilot phase, minor wording changes were made, and ambiguous items were revised to improve comprehensibility.
Assessment methods for cognitive function
Short-term memory assessment was used in the cognitive function section. The digit span (forward and backward) subtests of the Wechsler intelligence scale for children (WISC) were used to measure the capacity to store and process information in working memory. In the forward digit span test, orally presented lists of digits, ranging from 3 to 9 and increasing in length with each trial, were administered, and the participant was asked to recall them in the exact order presented. In the backward digit span test, the participant heard lists of digits ranging from 2 to 8, increasing in length with each trial, and was asked to recall them in reverse order. Each row contained two series of digits; therefore, each row was worth 2 points. If a participant correctly recalled a series of digits in a row, they received 1 point for that row. If either series was incorrectly recalled, the test was discontinued. Accordingly, the minimum score was 2 and the maximum was 14, ranging from very poor to very good. The reliability of the forward digit span test was reported to be 0.8, and the backward digit span test to be 0.68 [15].
Assessment methods for motor function
In this section, the agility and upper-body muscle strength of first-grade elementary school girls were evaluated. Agility was assessed using the 1-minute lateral jump test. For this purpose, an obstacle 5 cm high and 1 m long was placed in the middle of the designated area. To begin, the subject stood with their feet together on one side of the obstacle. Upon the “go” command, the subject jumped to the right and then returned to the starting position. The number of jumps performed in 1 minute was counted and recorded. Upper body muscle strength was assessed using the medicine ball throw test with a 1.5 kg ball for ages 7-9 and a 2.5 kg ball for ages 9-11. For this purpose, the subject stood behind a designated line with their feet shoulder-width apart. Then, they held the ball with both hands toward the center of their chest. The forearms were parallel to the ground. The subject threw the medicine ball forward with as much force as possible in a straight line. The distance of the throw was then recorded [16].
Statistical analysis
Descriptive statistics included Mean±SD, frequencies, and percentages. Normality was assessed using the Kolmogorov–Smirnov test. The Pearson correlation coefficients were applied as appropriate. Multiple linear regression analysis (enter method) was used. Missing data were handled using listwise deletion. Analyses were performed using SPSS software, version 22, with significance set at P<0.05.
Results
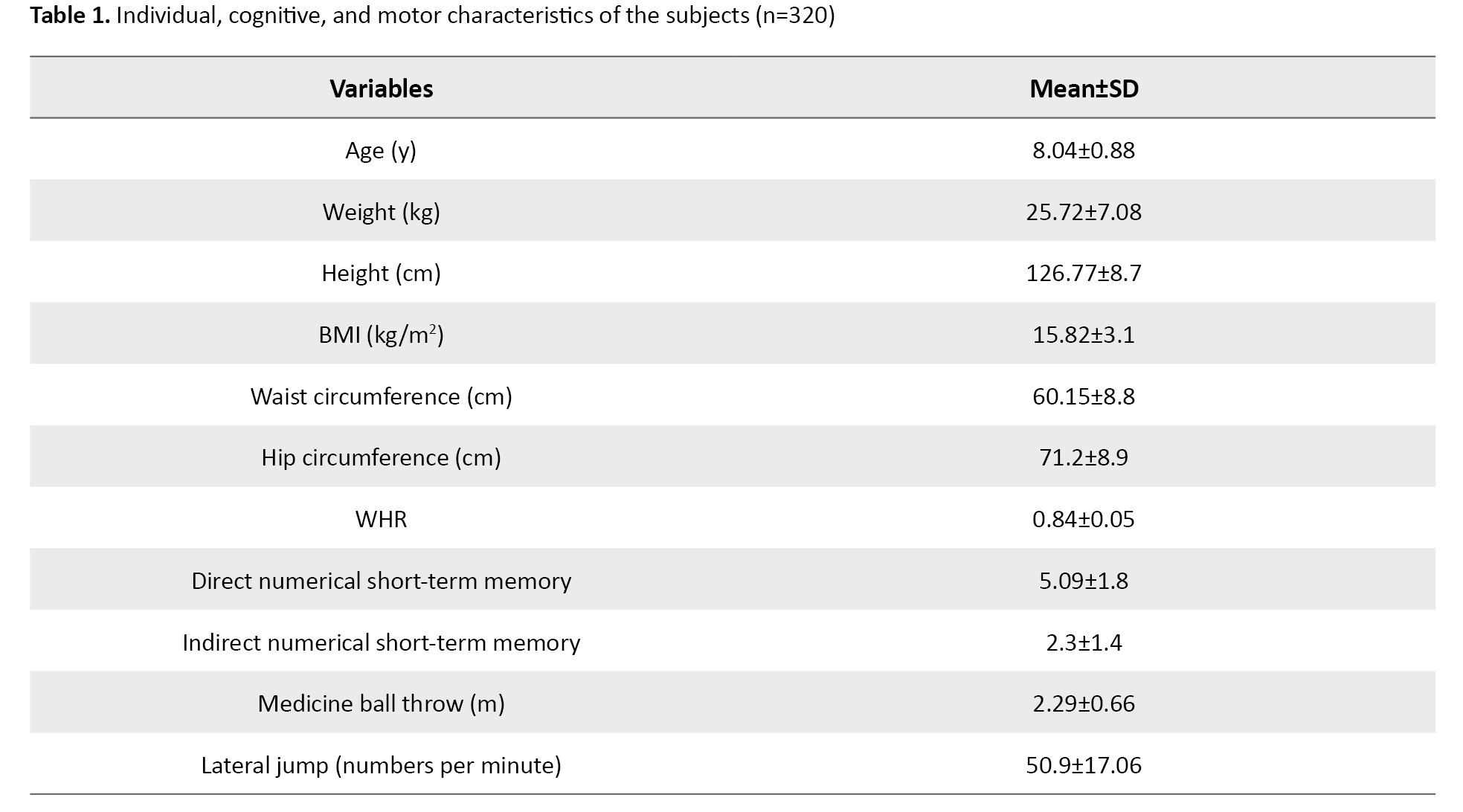
A total of 365 girls from an elementary school were initially recruited for the study. After excluding participants with incomplete questionnaires (n=31), parental consent withdrawal (n=9), or absence during cognitive or motor testing sessions (n=5), data from 320 participants were included in the final analysis. Participants had a mean age of 8.04±0.88 years. The mean body weight was 25.72±7.08 kg, the mean height was 126.77±8.7 cm, and the mean BMI was 15.82±3.10 kg/m². The mean waist circumference, hip circumference, and WHR were 60.15±8.8 cm, 71.2±8.9 cm, and 0.84±0.05, respectively. Descriptive statistics for cognitive and motor function variables are presented in Table 1.
Normality of continuous variables was assessed using the Kolmogorov–Smirnov test, and all variables met the assumptions for parametric statistical analyses (P>0.05).
Among participants, 67 students (20.9%) reported not usually eating breakfast before school, whereas 253(79.1%) reported eating breakfast. Only 196 students (61.3%) consumed breakfast on all five school days, while 35(10.8%) reported consuming breakfast only 2 to 3 days per week. Regarding breakfast composition, 226 students (70.6%) consumed bread as the main food item from the grains group, with a mean intake of 1.7 servings. Additionally, 189 students (59.1%) consumed cheese as the primary dairy product, with a mean intake of 1.1 servings. Consumption of other food groups, including meat and protein sources, fruits and vegetables, and fats and oils, was reported by less than 1% of participants. The most common breakfast combination was bread and cheese, providing an estimated energy intake of approximately 235 kcal, which is lower than recommended for girls aged 7–11 years.
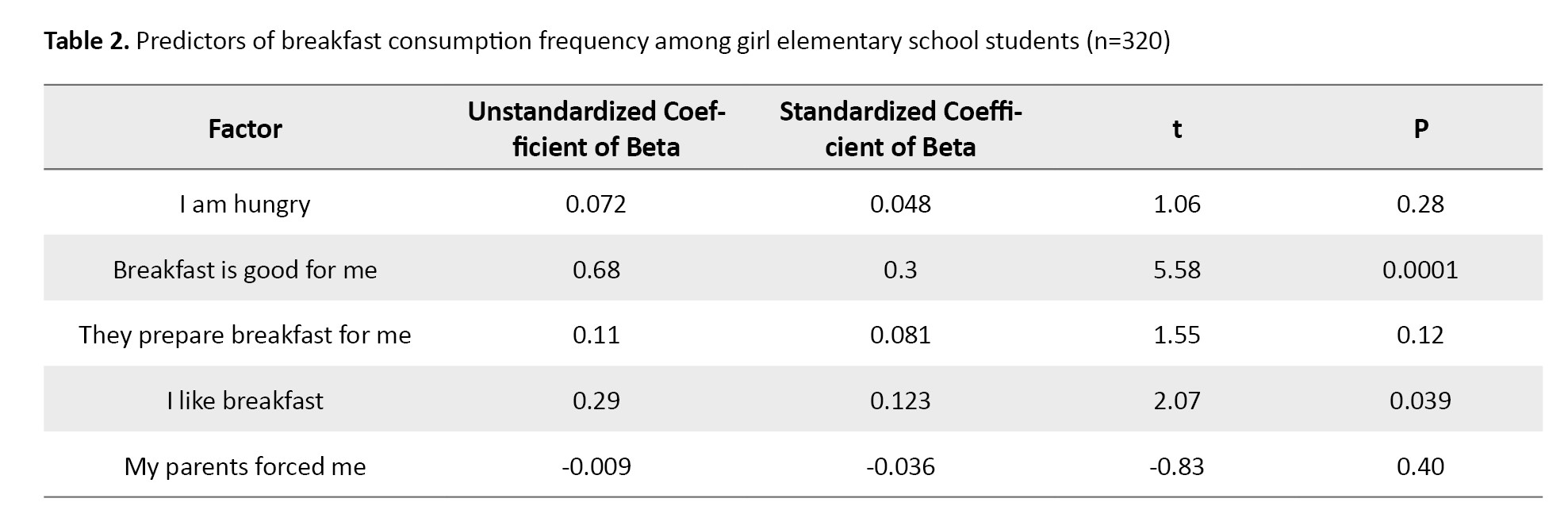
Multiple linear regression analysis was conducted to examine factors associated with breakfast consumption frequency. Among the examined factors, perceived health benefits of breakfast (β=0.3, P<0.001) and liking breakfast (β=0.12, P=0.039) were significant predictors of breakfast consumption. Other factors, including hunger, parental preparation, and parental pressure, were not significantly associated with breakfast consumption (Table 2).
Standardized regression coefficients are reported to facilitate interpretation.
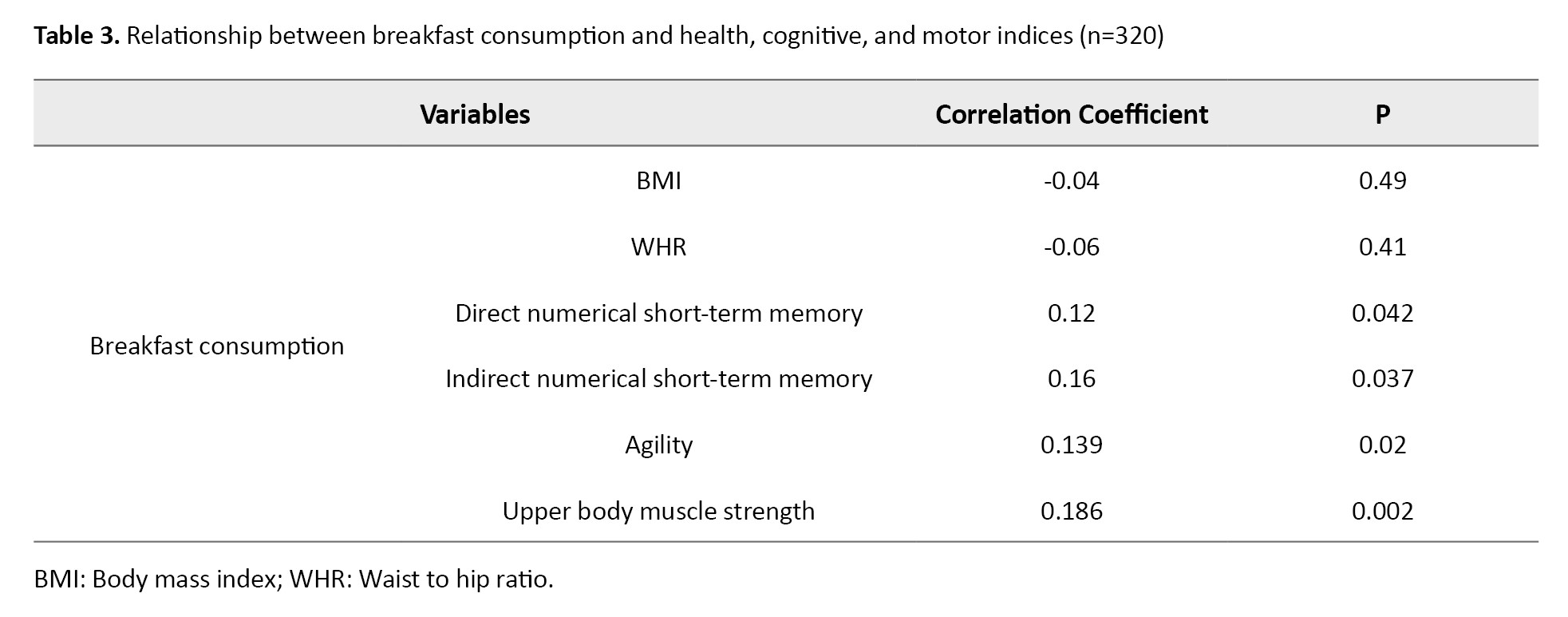
Pearson correlation analyses showed no significant association between breakfast consumption frequency and BMI (r=−0.04; 95% CI, −0.15%, 0.07%; P=0.49) or WHR (r=−0.06; 95% CI, −0.17%, 0.05%; P=0.41). However, breakfast consumption frequency was positively correlated with cognitive performance, including forward digit span (r=0.12; 95% CI, 0.01%, 0.23%; P=0.042) and backward digit span (r=0.16; 95% CI, 0.02%, 0.28%; P=0.037). Additionally, significant positive correlations were observed between breakfast consumption and agility (r=0.139; 95% CI, 0.02%, 0.25%; P=0.020) and upper body muscle strength (r=0.186; 95% CI, 0.06%, 0.3%; P=0.002). Although these associations were statistically significant, the effect sizes were small, indicating weak correlations. These findings are further illustrated in Table 3.
Discussion
The present study investigated breakfast consumption patterns and their associations with selected health indicators, as well as cognitive and motor function, among girl elementary school students aged 7–11 years studying in Qazvin. The discussion is structured around four key findings: breakfast consumption prevalence and quality, cognitive outcomes, motor performance, and anthropometric health indicators. The findings indicate that approximately one-fifth of participants (20.9%) regularly skipped breakfast on school days, while the majority did not, and those who did predominantly consumed bread and cheese. This prevalence of breakfast skipping is higher than that reported in several Western countries, where regular breakfast consumption among children often exceeds 75–85%. Still, it is comparable to or slightly higher than rates reported in previous Iranian studies, which range from approximately 15% to over 30% depending on region and age group. Terry et al. (2020) also reported that roughly 87% of children aged 6-11 years in the United States regularly consumed breakfast, while 13% had irregular breakfast consumption or did not consume breakfast [17]. However, Gutkowska et al. (2025) reported that approximately two-thirds of the children were daily breakfast consumers (7 d/wk), 24% were breakfast skippers (0–3 d/wk), and 14% had irregular breakfast consumption (4–6 d/wk). [3]. These differences may reflect contextual factors such as socioeconomic status, parental work schedules, food availability, and cultural norms regarding breakfast preparation. What people eat for breakfast varies from country to country. In Western countries, such as the United Kingdom (Great Britain), breakfast typically provides all the necessary nutrients. Moreover, they present an appealing appearance to consumers, particularly children. However, in Asian countries, breakfast is usually a quick and easy meal. Less emphasis is placed on the colors and nutrients present in the food. Thus, their breakfast is typically determined by preparation time and difficulty [18, 19].
Notably, breakfast quality in the present study was limited, with minimal intake of fruits, vegetables, and protein-rich foods. This finding suggests that breakfast consumption alone may not be sufficient to confer optimal nutritional benefits and that the composition of breakfast should be considered when evaluating its health and functional implications [20].
Breakfast consumption frequency was positively associated with short-term and working memory, as measured by forward and backward digit span tests. Although the observed correlations were modest, they are consistent with previous evidence linking regular breakfast consumption to improved cognitive performance and academic outcomes in children. In a review study, Ong et al. (2024) stated that most studies have concluded that regular breakfast consumption, compared to irregular consumption, leads to better school performance. Before the implementation of the free school breakfast program, 33% of students were at risk of malnutrition, which led to poor school performance. This condition included poor punctuality and attendance, as well as increased behavioral problems [19]. Several biological and psychological mechanisms may explain this association. Breakfast consumption may replenish glucose levels after overnight fasting, supporting brain energy metabolism and neurotransmitter function, which are essential for attention, memory, and information processing [21]. In addition, regular breakfast consumption may contribute to improved mood, alertness, and classroom engagement, indirectly enhancing cognitive performance [22, 23].
The present study also demonstrated weak but significant positive associations between breakfast consumption and motor performance indicators, including agility and upper body muscular strength. These findings align with some previous studies reporting better physical fitness among children who regularly consume breakfast. Gao et al. (2023) also reported a positive and significant correlation between breakfast frequency and physical fitness indicators, including grip strength and the 20-m shuttle run, among students [12]. Adequate morning energy intake may enhance neuromuscular coordination and physical readiness during school hours. However, physical fitness is influenced by multiple factors, including habitual physical activity, sports participation, and overall diet quality, which were not fully controlled for in this study and may partially explain the modest effect sizes observed.
In contrast to cognitive and motor outcomes, breakfast consumption was not significantly associated with BMI or WHR. Consistent with the present research, Al-Hazzaa et al. (2020) also reported no correlation between obesity levels and breakfast consumption [24]. Moreover, Annan et al. (2020) reported no significant correlation between daily breakfast consumption and BMI [5]. Several hypotheses may explain this finding. First, anthropometric indicators reflect long-term energy balance, whereas breakfast consumption was assessed as a behavioral frequency measure without precise quantification of total daily energy intake [25]. Second, the generally low energy content and limited nutritional diversity of breakfast observed in this study may have attenuated any potential association with body composition [26, 27]. Third, unmeasured confounding factors such as physical activity levels, sedentary behavior, sleep patterns, and socioeconomic status may have influenced anthropometric outcomes [25]. These explanations are consistent with previous studies reporting null or inconsistent associations between breakfast consumption and obesity-related indicators in cross-sectional designs [25-27].
Conclusion
In conclusion, the present study found that a substantial proportion of girl elementary school students in Qazvin regularly skip breakfast, and that breakfast quality is generally limited in terms of nutritional diversity. While breakfast consumption was not significantly associated with physical health indicators, it showed positive associations with cognitive and motor performance, albeit with small effect sizes. These findings underscore the potential role of regular and nutritionally adequate breakfast consumption in supporting children’s functional development. School-based breakfast programs and parent-focused nutrition education initiatives may be practical strategies to improve children’s breakfast habits. Future longitudinal and interventional studies are needed to confirm causal relationships, assess the impact of breakfast quality, and inform evidence-based public health policies to promote child health and development.
Study limitations
This study has several limitations that must be considered when interpreting the results—first, the cross-sectional design limits causal inference. Second, the reliance on self- and parent-reported dietary data may have introduced recall and reporting bias. Third, the sample was limited to female students from Qazvin. Therefore, the generalizability of the findings to boys, other age groups, or different geographical regions may be limited. Fourth, although some confounders were controlled for, factors such as precise socioeconomic status, parental education, and physical activity levels were not fully measured or adjusted for and may have acted as residual confounders. Nevertheless, the study also has notable strengths, including a relatively large sample size, the simultaneous assessment of cognitive and motor outcomes, and the use of standardized measurement protocols.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Qazvin University of Medical Sciences, Qazvin, Iran (Code: IR.QUMS.REC.1403.001). Written informed consent was obtained from parents or legal guardians, and verbal assent was obtained from all participating children before data collection. Participation was voluntary, and confidentiality of all data was ensured. Informed consent for anonymous publication of data was obtained from all participants through their parents or legal guardians.
Funding
This research received no grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, and initial draft preparation: Nahid Ebrahimi and Hassan Pourrazi; Data collection, data analysis, and interpretation: Nahid Ebrahimi and Hassan Pourrazi; Review, editing, and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to express their sincere gratitude to the Qazvin Department of Education, school principals, and teaching staff for their valuable cooperation in conducting this study. The authors also extend their appreciation to the parents and students who participated in this research for their time and cooperation.
Proper nutrition and adequate physical activity are fundamental determinants of optimal growth and health among school-aged children [1]. Recent global evidence indicates that unhealthy dietary behaviors and sedentary lifestyles contribute substantially to childhood overweight and obesity, which remain major public health challenges worldwide [2, 3]. Childhood and early school years represent a critical developmental window during which health-related behaviors are established and often track into adolescence and adulthood, thereby influencing long-term health outcomes [4, 5]. Childhood overweight and obesity are associated with adverse cardiometabolic consequences, including elevated blood pressure, dyslipidemia, and insulin resistance, many of which may persist into adulthood [6, 7]. While physical activity plays a crucial role in energy balance, dietary habits are equally important determinants of body weight and overall health status. Previous studies have shown that diet quality, independent of total energy intake, may significantly influence body weight and body mass index (BMI) in children [8]. Given the fundamental role of schools in children’s daily lives, school-based nutrition interventions, particularly those involving families, have been identified as effective strategies for promoting healthy eating behaviors and active lifestyles [8, 9]. Breakfast is commonly regarded as the first meal of the day and has been linked to several beneficial health and functional outcomes. Regular breakfast consumption has been associated with improved dietary quality, more favorable weight status, and better academic and cognitive performance among children and adolescents [10, 11].
Additionally, recent evidence suggests a positive association between breakfast consumption frequency and physical fitness indicators, such as cardiorespiratory endurance and muscular strength [12]. Nevertheless, findings across studies are not entirely consistent, and the mechanisms underlying these associations remain incompletely understood. Patterns of breakfast consumption vary across populations and are influenced by socioeconomic, cultural, and environmental factors. Studies conducted in different regions have reported a higher prevalence of breakfast skipping among girls, particularly those from lower socioeconomic backgrounds [11]. In Iran, several studies have examined breakfast consumption habits among school-aged children and adolescents, reporting considerable variability in consumption patterns and identifying factors such as time constraints, lack of appetite, and limited food availability as common reasons for breakfast omission [13, 14]. However, most Iranian studies have focused primarily on the prevalence of breakfast consumption or its association with obesity and academic performance, with limited attention to breakfast quality and functional outcomes. Moreover, there is a paucity of localized evidence examining the quantity and quality of breakfast consumption and their associations with anthropometric and functional outcomes among elementary school girls. In the present study, health indicators refer specifically to anthropometric measures commonly used to assess nutritional status and obesity-related health risks in children, including body weight, BMI, and waist-to-hip ratio (WHR). Therefore, this study aims to assess breakfast consumption status, including its frequency, quantity, and quality, and to investigate its association with selected physical health indicators as well as cognitive and motor function among girls aged 7–11 living in Qazvin, Iran. The findings of this study may provide valuable evidence for school administrators, public health practitioners, nutrition professionals, and policymakers to inform the development of targeted school-based nutrition programs and family-centered interventions to improve children’s health and functional outcomes.
Materials and Methods
This cross-sectional, descriptive–analytical correlational study was conducted among girl elementary school students studying in Qazvin, Iran, during the 2023–2024 academic year. The source population consisted of approximately 8000 girl students aged 7–11 years enrolled in public and private elementary schools.
The sample size was calculated using Cochran’s formula for correlation studies, assuming a confidence level of 95%, a statistical power of 80%, and an anticipated moderate correlation coefficient (r=0.15) based on previous similar studies. The minimum required sample size was estimated at 320 participants. To account for potential non-response and incomplete questionnaires, 365 students were initially recruited. A multistage cluster sampling method was employed. First, 2 educational districts in Qazvin were randomly selected as clusters. From each district, 1 public and 1 private elementary school were randomly chosen. Within each selected school, students were selected by simple random sampling using student identification numbers. Of the 365 recruited students, 45 were excluded due to incomplete questionnaires (n=31), withdrawal of consent (n=9), or absence during cognitive or motor testing sessions (n=5). Therefore, data from 320 participants were included in the final analysis, corresponding to a questionnaire non-completion rate of approximately 12.5%. No systematic differences were observed between included and excluded participants in terms of age or school type.
The inclusion criteria were girl students aged 7–11 years enrolled in elementary schools whose parents provided written informed consent. The exclusion criteria included any diagnosed chronic illness (e.g. diabetes, cardiovascular disease, and asthma), neurological or developmental disorders, use of medications affecting growth or cognitive function, adherence to medically prescribed dietary regimens, or unwillingness of the child or parent to participate.
Before the main study, a pilot study was conducted with 30 girl elementary school students from one school, which was not included in the final sample. The pilot aimed to assess the feasibility, clarity of questionnaire items, assessment duration, and logistical procedures. Based on feedback from parents and children, minor wording revisions were made to simplify questions related to breakfast quantity and food types, and the sequence of questionnaire sections was adjusted to improve comprehension.
Written informed consent was obtained from parents or legal guardians, and verbal assent was obtained from all participating children before data collection. Participation was voluntary, and confidentiality of all data was ensured. Body weight was measured twice using a calibrated Seca digital scale with participants barefoot and wearing light clothing; the mean value was recorded to the nearest 0.2 kg. Height was measured twice using a Seca stadiometer with participants standing upright, barefoot, heels together, and head positioned in the Frankfurt plane; the mean value was recorded to the nearest 0.5 cm. BMI was calculated as weight (kg)/height² (m²). Waist and hip circumferences were measured twice using a non-elastic tape in a standing position, and the mean values were used to calculate WHR.
Assessment methods for breakfast consumption status
Breakfast consumption was assessed using a researcher-developed questionnaire completed by students with parental assistance. The questionnaire consisted of 3 sections. The first section collected demographic and socioeconomic information, including age, parental education level, household income, and parental employment status. The second section assessed breakfast consumption patterns, including frequency, quantity, and types of foods consumed. The third section examined factors influencing breakfast consumption or omission among girls aged 7–11 years.
Breakfast consumption frequency was assessed using a 5-point Likert-type scale, reflecting the number of days breakfast was consumed at home during a typical week, with response options ranging from 0 days (no breakfast at home) to 4–5 days (regular breakfast at home). This variable was treated as an ordinal measure. Factors influencing breakfast consumption or non-consumption (including perceived health benefits of breakfast, liking breakfast, hunger, parental preparation, and parental pressure) were assessed using a similar 5-point Likert-type scale ranging from strongly disagree to agree strongly. No composite breakfast consumption score was calculated; therefore, each item was analyzed separately according to its measurement level.
Content validity of the questionnaire was established by an expert panel consisting of specialists in nutrition and public health. The content validity index (CVI) for the questionnaire was acceptable. Internal consistency reliability was assessed using the Cronbach α, yielding a coefficient of 0.81. Before the main study, the questionnaire was pilot-tested among 30 girl elementary school students from one school not included in the final sample to evaluate clarity, feasibility, and completion time. Based on feedback from the pilot phase, minor wording changes were made, and ambiguous items were revised to improve comprehensibility.
Assessment methods for cognitive function
Short-term memory assessment was used in the cognitive function section. The digit span (forward and backward) subtests of the Wechsler intelligence scale for children (WISC) were used to measure the capacity to store and process information in working memory. In the forward digit span test, orally presented lists of digits, ranging from 3 to 9 and increasing in length with each trial, were administered, and the participant was asked to recall them in the exact order presented. In the backward digit span test, the participant heard lists of digits ranging from 2 to 8, increasing in length with each trial, and was asked to recall them in reverse order. Each row contained two series of digits; therefore, each row was worth 2 points. If a participant correctly recalled a series of digits in a row, they received 1 point for that row. If either series was incorrectly recalled, the test was discontinued. Accordingly, the minimum score was 2 and the maximum was 14, ranging from very poor to very good. The reliability of the forward digit span test was reported to be 0.8, and the backward digit span test to be 0.68 [15].
Assessment methods for motor function
In this section, the agility and upper-body muscle strength of first-grade elementary school girls were evaluated. Agility was assessed using the 1-minute lateral jump test. For this purpose, an obstacle 5 cm high and 1 m long was placed in the middle of the designated area. To begin, the subject stood with their feet together on one side of the obstacle. Upon the “go” command, the subject jumped to the right and then returned to the starting position. The number of jumps performed in 1 minute was counted and recorded. Upper body muscle strength was assessed using the medicine ball throw test with a 1.5 kg ball for ages 7-9 and a 2.5 kg ball for ages 9-11. For this purpose, the subject stood behind a designated line with their feet shoulder-width apart. Then, they held the ball with both hands toward the center of their chest. The forearms were parallel to the ground. The subject threw the medicine ball forward with as much force as possible in a straight line. The distance of the throw was then recorded [16].
Statistical analysis
Descriptive statistics included Mean±SD, frequencies, and percentages. Normality was assessed using the Kolmogorov–Smirnov test. The Pearson correlation coefficients were applied as appropriate. Multiple linear regression analysis (enter method) was used. Missing data were handled using listwise deletion. Analyses were performed using SPSS software, version 22, with significance set at P<0.05.
Results
A total of 365 girls from an elementary school were initially recruited for the study. After excluding participants with incomplete questionnaires (n=31), parental consent withdrawal (n=9), or absence during cognitive or motor testing sessions (n=5), data from 320 participants were included in the final analysis. Participants had a mean age of 8.04±0.88 years. The mean body weight was 25.72±7.08 kg, the mean height was 126.77±8.7 cm, and the mean BMI was 15.82±3.10 kg/m². The mean waist circumference, hip circumference, and WHR were 60.15±8.8 cm, 71.2±8.9 cm, and 0.84±0.05, respectively. Descriptive statistics for cognitive and motor function variables are presented in Table 1.
Normality of continuous variables was assessed using the Kolmogorov–Smirnov test, and all variables met the assumptions for parametric statistical analyses (P>0.05).
Among participants, 67 students (20.9%) reported not usually eating breakfast before school, whereas 253(79.1%) reported eating breakfast. Only 196 students (61.3%) consumed breakfast on all five school days, while 35(10.8%) reported consuming breakfast only 2 to 3 days per week. Regarding breakfast composition, 226 students (70.6%) consumed bread as the main food item from the grains group, with a mean intake of 1.7 servings. Additionally, 189 students (59.1%) consumed cheese as the primary dairy product, with a mean intake of 1.1 servings. Consumption of other food groups, including meat and protein sources, fruits and vegetables, and fats and oils, was reported by less than 1% of participants. The most common breakfast combination was bread and cheese, providing an estimated energy intake of approximately 235 kcal, which is lower than recommended for girls aged 7–11 years.
Multiple linear regression analysis was conducted to examine factors associated with breakfast consumption frequency. Among the examined factors, perceived health benefits of breakfast (β=0.3, P<0.001) and liking breakfast (β=0.12, P=0.039) were significant predictors of breakfast consumption. Other factors, including hunger, parental preparation, and parental pressure, were not significantly associated with breakfast consumption (Table 2).
Standardized regression coefficients are reported to facilitate interpretation.
Pearson correlation analyses showed no significant association between breakfast consumption frequency and BMI (r=−0.04; 95% CI, −0.15%, 0.07%; P=0.49) or WHR (r=−0.06; 95% CI, −0.17%, 0.05%; P=0.41). However, breakfast consumption frequency was positively correlated with cognitive performance, including forward digit span (r=0.12; 95% CI, 0.01%, 0.23%; P=0.042) and backward digit span (r=0.16; 95% CI, 0.02%, 0.28%; P=0.037). Additionally, significant positive correlations were observed between breakfast consumption and agility (r=0.139; 95% CI, 0.02%, 0.25%; P=0.020) and upper body muscle strength (r=0.186; 95% CI, 0.06%, 0.3%; P=0.002). Although these associations were statistically significant, the effect sizes were small, indicating weak correlations. These findings are further illustrated in Table 3.
Discussion
The present study investigated breakfast consumption patterns and their associations with selected health indicators, as well as cognitive and motor function, among girl elementary school students aged 7–11 years studying in Qazvin. The discussion is structured around four key findings: breakfast consumption prevalence and quality, cognitive outcomes, motor performance, and anthropometric health indicators. The findings indicate that approximately one-fifth of participants (20.9%) regularly skipped breakfast on school days, while the majority did not, and those who did predominantly consumed bread and cheese. This prevalence of breakfast skipping is higher than that reported in several Western countries, where regular breakfast consumption among children often exceeds 75–85%. Still, it is comparable to or slightly higher than rates reported in previous Iranian studies, which range from approximately 15% to over 30% depending on region and age group. Terry et al. (2020) also reported that roughly 87% of children aged 6-11 years in the United States regularly consumed breakfast, while 13% had irregular breakfast consumption or did not consume breakfast [17]. However, Gutkowska et al. (2025) reported that approximately two-thirds of the children were daily breakfast consumers (7 d/wk), 24% were breakfast skippers (0–3 d/wk), and 14% had irregular breakfast consumption (4–6 d/wk). [3]. These differences may reflect contextual factors such as socioeconomic status, parental work schedules, food availability, and cultural norms regarding breakfast preparation. What people eat for breakfast varies from country to country. In Western countries, such as the United Kingdom (Great Britain), breakfast typically provides all the necessary nutrients. Moreover, they present an appealing appearance to consumers, particularly children. However, in Asian countries, breakfast is usually a quick and easy meal. Less emphasis is placed on the colors and nutrients present in the food. Thus, their breakfast is typically determined by preparation time and difficulty [18, 19].
Notably, breakfast quality in the present study was limited, with minimal intake of fruits, vegetables, and protein-rich foods. This finding suggests that breakfast consumption alone may not be sufficient to confer optimal nutritional benefits and that the composition of breakfast should be considered when evaluating its health and functional implications [20].
Breakfast consumption frequency was positively associated with short-term and working memory, as measured by forward and backward digit span tests. Although the observed correlations were modest, they are consistent with previous evidence linking regular breakfast consumption to improved cognitive performance and academic outcomes in children. In a review study, Ong et al. (2024) stated that most studies have concluded that regular breakfast consumption, compared to irregular consumption, leads to better school performance. Before the implementation of the free school breakfast program, 33% of students were at risk of malnutrition, which led to poor school performance. This condition included poor punctuality and attendance, as well as increased behavioral problems [19]. Several biological and psychological mechanisms may explain this association. Breakfast consumption may replenish glucose levels after overnight fasting, supporting brain energy metabolism and neurotransmitter function, which are essential for attention, memory, and information processing [21]. In addition, regular breakfast consumption may contribute to improved mood, alertness, and classroom engagement, indirectly enhancing cognitive performance [22, 23].
The present study also demonstrated weak but significant positive associations between breakfast consumption and motor performance indicators, including agility and upper body muscular strength. These findings align with some previous studies reporting better physical fitness among children who regularly consume breakfast. Gao et al. (2023) also reported a positive and significant correlation between breakfast frequency and physical fitness indicators, including grip strength and the 20-m shuttle run, among students [12]. Adequate morning energy intake may enhance neuromuscular coordination and physical readiness during school hours. However, physical fitness is influenced by multiple factors, including habitual physical activity, sports participation, and overall diet quality, which were not fully controlled for in this study and may partially explain the modest effect sizes observed.
In contrast to cognitive and motor outcomes, breakfast consumption was not significantly associated with BMI or WHR. Consistent with the present research, Al-Hazzaa et al. (2020) also reported no correlation between obesity levels and breakfast consumption [24]. Moreover, Annan et al. (2020) reported no significant correlation between daily breakfast consumption and BMI [5]. Several hypotheses may explain this finding. First, anthropometric indicators reflect long-term energy balance, whereas breakfast consumption was assessed as a behavioral frequency measure without precise quantification of total daily energy intake [25]. Second, the generally low energy content and limited nutritional diversity of breakfast observed in this study may have attenuated any potential association with body composition [26, 27]. Third, unmeasured confounding factors such as physical activity levels, sedentary behavior, sleep patterns, and socioeconomic status may have influenced anthropometric outcomes [25]. These explanations are consistent with previous studies reporting null or inconsistent associations between breakfast consumption and obesity-related indicators in cross-sectional designs [25-27].
Conclusion
In conclusion, the present study found that a substantial proportion of girl elementary school students in Qazvin regularly skip breakfast, and that breakfast quality is generally limited in terms of nutritional diversity. While breakfast consumption was not significantly associated with physical health indicators, it showed positive associations with cognitive and motor performance, albeit with small effect sizes. These findings underscore the potential role of regular and nutritionally adequate breakfast consumption in supporting children’s functional development. School-based breakfast programs and parent-focused nutrition education initiatives may be practical strategies to improve children’s breakfast habits. Future longitudinal and interventional studies are needed to confirm causal relationships, assess the impact of breakfast quality, and inform evidence-based public health policies to promote child health and development.
Study limitations
This study has several limitations that must be considered when interpreting the results—first, the cross-sectional design limits causal inference. Second, the reliance on self- and parent-reported dietary data may have introduced recall and reporting bias. Third, the sample was limited to female students from Qazvin. Therefore, the generalizability of the findings to boys, other age groups, or different geographical regions may be limited. Fourth, although some confounders were controlled for, factors such as precise socioeconomic status, parental education, and physical activity levels were not fully measured or adjusted for and may have acted as residual confounders. Nevertheless, the study also has notable strengths, including a relatively large sample size, the simultaneous assessment of cognitive and motor outcomes, and the use of standardized measurement protocols.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Qazvin University of Medical Sciences, Qazvin, Iran (Code: IR.QUMS.REC.1403.001). Written informed consent was obtained from parents or legal guardians, and verbal assent was obtained from all participating children before data collection. Participation was voluntary, and confidentiality of all data was ensured. Informed consent for anonymous publication of data was obtained from all participants through their parents or legal guardians.
Funding
This research received no grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, and initial draft preparation: Nahid Ebrahimi and Hassan Pourrazi; Data collection, data analysis, and interpretation: Nahid Ebrahimi and Hassan Pourrazi; Review, editing, and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to express their sincere gratitude to the Qazvin Department of Education, school principals, and teaching staff for their valuable cooperation in conducting this study. The authors also extend their appreciation to the parents and students who participated in this research for their time and cooperation.
References
- Zhou S, Zhao H, Xiao Y, Li J, Huang Q, Zhang Y, et al. Association of breakfast food types with dietary knowledge, attitudes, and practices among school-aged children. Nutrients. 2025; 17(15):2424. [DOI:10.3390/nu17152424] [PMID]
- Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of population-based measurement studies. Lancet. 2017; 390(10113):2627-42. [DOI:10.1016/S0140-6736(17)32129-3] [PMID]
- Gutkowska K, Wierzbicka E, Madej D, Czarniecka-Skubina E, Hamulka J. Breakfast frequency, lifestyle-related factors and their association with body weight status among Polish primary school children aged 10 to 12 years. Nutrition Journal. 2025; 24(1):160. [DOI:10.1186/s12937-025-01231-4] [PMID]
- Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas. 2011; 70(3):266-84. [DOI:10.1016/j.maturitas.2011.08.005] [PMID]
- Annan RA, Sowah SA, Apprey C, Agyapong NA, Okonogi S, Yamauchi T, et al. Relationship between breakfast consumption, BMI status and physical fitness of Ghanaian school-aged children. BMC Nutrition. 2020; 6(1):19. [DOI:10.1186/s40795-020-00344-9] [PMID]
- Cabral S, Soares L, Faria AL. Obesity in childhood and adolescence: A review. Biomedical Journal of Scientific and Technical Research. 2023; 51(3):42704-9. [DOI:10.26717/BJSTR.2023.51.008102]
- Caprio S, Santoro N, Weiss R. Childhood obesity and the associated rise in cardiometabolic complications. Nature Metabolism. 2020; 2(3):223-32. [DOI:10.1038/s42255-020-0183-z] [PMID]
- Kocaadam-Bozkurt B, Sözlü S, Macit-Çelebi MS. Exploring how parenting influences children’s nutritional status, physical activity, and BMI. Frontiers in Nutrition. 2023; 9:1096182. [DOI:10.3389/fnut.2022.1096182] [PMID]
- Baldinger N, Krebs A, Müller R, Aeberli I. Swiss children consuming breakfast regularly have better motor functional skills and are less overweight than breakfast skippers. Journal of The American College of Nutrition. 2012; 31(2):87-93. [DOI:10.1080/07315724.2012.10720013] [PMID]
- Adonu RE, Amoah M, Saah FI. Breakfast intake and associated factors and barriers among tertiary institution students in Ghana. BMC Nutrition. 2023; 9(1):7. [DOI:10.1186/s40795-023-00672-6] [PMID]
- Hovdenak IM, Helleve A, Wolden IE, Bere E. Socioeconomic inequality in breakfast skipping among Norwegian adolescents. Nutrition Journal. 2024; 23(1):94. [DOI:10.1186/s12937-024-00998-2] [PMID]
- Gao L, Chang ZM, Luo SC, Meng Y, Liu C. Correlation between physical fitness and frequency of breakfast consumption of middle school students. Chinese Journal of School Health. 2023; 44(2):261-65. [Link]
- Soheilipour F, Salehiniya H, Farajpourkh M, Pishgahroudsari M. Breakfast habits, nutritional status and their relationship with academic performance in elementary school students of Tehran, Iran. Medicine and Pharmacy Reports. 2019; 92(1):52-6. [DOI:10.15386/cjmed-956] [PMID]
- Azadbakht L, Izadi V, Esmaillzadeh A. The importance of the first mealtime in prevalence of overweightness and obesity among female adolescents in Isfahan. International Journal of School Health. 2014; 1(3):1-6. [DOI:10.17795/intjsh-24547]
- Pham T, Archibald LM. Are children performing better on the digit span backward task than the digit span forward task? American Journal of Speech-Language Pathology. 2023; 32(5):2311-21. [DOI:10.1044/2023_AJSLP-22-00394] [PMID]
- González-Devesa D, Varela S, Diz-Gómez JC, López-Amoedo D, Ayán-Pérez C. Reliability and validity of the medicine ball throw test in children and adolescents: A systematic review and meta-analysis. Kinesiology. 2025; 57(1):122-35. [DOI:10.26582/k.57.1.11]
- Terry AL, Wambogo E, Ansai N, Ahluwalia N. Breakfast intake among children and adolescents: United States, 2015-2018. NCHS Data Brief. 2020; 386:1-8. [Link]
- Motlagh ME, Taheri M, Ghadimi R, Shirvani DN. [Breakfast and snack status among the students of Iranian ethnicities (Persian)]. Iranian Journal of Nutrition Sciences and Food Technology. 2017; 12(1):29-36. [Link]
- Ong RT, Lao S, Seow Sh, Shrikant Dave V, Ling M. Systematic review of PubMed articles prior to 2023 on effects of breakfast on school performance. Medicon Medical Sciences. 2024; 6(1):11-25. [Link]
- Delvarianzadeh M, Saadat S, Ebrahimi MH. Assessment of nutritional status and its related factors among Iranian university students: A cross-sectional study. Iranian Journal of Health Sciences. 2016; 4(4):56-68. [DOI:10.18869/acadpub.jhs.4.4.56]
- Betts JA, Chowdhury EA, Gonzalez JT, Richardson JD, Tsintzas K, Thompson D. Is breakfast the most important meal of the day? Proceedings of the Nutrition Society. 2016; 75(4):464-74. [DOI:10.1017/S0029665116000318] [PMID]
- Yao J, Liu Y, Zhou S. Effect of eating breakfast on cognitive development of elementary and middle school students. Medical Science Monitor. 2019; 25:8843. [DOI:10.12659/MSM.920459] [PMID]
- López-Gil JF, Tully MA, Cristi-Montero C, Brazo-Sayavera J, Gaya AR, Calatayud J, et al. Is the frequency of breakfast consumption associated with life satisfaction in children and adolescents? Nutrition Journal. 2024; 23(1):78. [DOI:10.1186/s12937-024-00979-5] [PMID]
- Al-Hazzaa HM, Al-Rasheedi AA, Alsulaimani RA, Jabri L. Anthropometric, familial- and lifestyle-related characteristics of school children skipping breakfast in Saudi Arabia. Nutrients. 2020; 12(12):3668. [DOI:10.3390/nu12123668] [PMID]
- Sampasa-Kanyinga H, Hamilton HA, Chaput JP. Movement behaviours, breakfast consumption, and fruit and vegetable intake among adolescents. Journal of Activity, Sedentary and Sleep Behaviors. 2022; 1(1):4. [DOI:10.1186/s44167-022-00001-5] [PMID]
- Yaguchi-Tanaka Y, Tabuchi T. Skipping breakfast and subsequent overweight or obesity in children: A nationwide prospective study in Japan. Journal of Epidemiology. 2021; 31(7):417-25. [DOI:10.2188/jea.JE20200266] [PMID]
- Sila S, Ilić A, Mišigoj-Duraković M, Sorić M, Radman I, Šatalić Z. Obesity in adolescents who skip breakfast is not associated with physical activity. Nutrients. 2019; 11(10):2511. [DOI:10.3390/nu11102511] [PMID]
Type of Study: Original Article |
Subject:
Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
