

Volume 14, Issue 1 (Winter 2026)
Iran J Health Sci 2026, 14(1): 65-74 |
Back to browse issues page


Ethics code: IR.MAZUMS.IMAMHOSPITAL.REC. 1402.101
Clinical trials code: 1
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zarrinkamar M, Alinejad E, Kashi Z, Geran M, Khosravi P, Arab R K et al . Assessment of Poor Glycemic Control and Associated Factors in Type 2 Diabetes Patients at Comprehensive Health Centers, Qaemshahr City, Iran, in 2023. Iran J Health Sci 2026; 14 (1) :65-74
URL: http://jhs.mazums.ac.ir/article-1-1056-en.html
URL: http://jhs.mazums.ac.ir/article-1-1056-en.html
Maryam Zarrinkamar 

 , Elham Alinejad , Zahra Kashi , Mojgan Geran * , Pejman Khosravi , Roghaye Khatoon Arab , Mohammad Khademloo
, Elham Alinejad , Zahra Kashi , Mojgan Geran * , Pejman Khosravi , Roghaye Khatoon Arab , Mohammad Khademloo
, Elham Alinejad , Zahra Kashi , Mojgan Geran * , Pejman Khosravi , Roghaye Khatoon Arab , Mohammad Khademloo
Department of Family Medicine, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran. & Diabetes Research Center, Institute of Herbal Medicines and Metabolic Disorders, Mazandaran University of Medical Sciences, Sari, Iran. , moj1357geran@gmail.com
Keywords: Type 2 diabetes mellitus (T2DM), Glycemic control, Glycosylated hemoglobin (HbA1c), Medication adherence
Full-Text [PDF 841 kb]
(252 Downloads)
| Abstract (HTML) (711 Views)
References
Full-Text: (161 Views)
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Three out of every 4 people with diabetes (79%) live in low- and middle-income countries. Diabetes is the seventh leading cause of death in the United States and is consistently among the top 10 causes of death in Iran [1]. In Iran, the prevalence of T2DM is 9.6%, and about 5 million adults with diabetes live in the country. Iran is one of the countries in the region with the highest number of people with diabetes, and it is predicted that this number will double by 2045 [2].
The prevalence data is slightly outdated (estimates indicate that over 135 million adults worldwide were affected in 1993, a number projected to reach 300 million by 2025 [1].
Despite advances in treatment, glycemic control remains suboptimal in a significant proportion of patients, leading to increased risk of acute and chronic complications such as cardiovascular disease, nephropathy, neuropathy, and retinopathy. Between 40% and 60% of patients worldwide have poorly controlled diabetes. Although blood glucose control is the main goal of treatment, it is not achieved in most patients [2, 3].
A complex interplay of factors, including genetic predisposition, environmental conditions, lifestyle, socioeconomic status, and patient adherence to treatment regimens, influences poor glycemic control. Studies have identified age, gender, duration of diabetes, BMI, educational level, and family history as important contributors to glycemic outcomes [4, 5].
Moreover, self-care behaviors, encompassing medication adherence, dietary management, physical activity, and regular monitoring, are critical determinants of successful diabetes management [6]. However, research indicates that, despite a considerable proportion of patients demonstrating medication adherence, actual self-care practices remain inadequate, highlighting a gap in comprehensive diabetes management education and support [7]. This gap is of particular concern in low- and middle-income settings, where healthcare resources are limited, and the burden of diabetes complications is rising.
Despite extensive global and national efforts to improve diabetes management, glycemic control remains suboptimal in a substantial proportion of patients, particularly in low- and middle-income countries. Although numerous studies have examined predictors of poor glycemic control, most available evidence is either outdated, limited to specific subgroups, or lacks a comprehensive assessment of both medication adherence and self-care behaviors simultaneously. Moreover, the majority of regional studies in Iran have focused on hospital-based populations, with limited data available from primary care and community health centers where most patients with type 2 diabetes routinely receive care. In Qaemshahr City, Iran, despite the high and growing burden of diabetes, no recent study has systematically evaluated the combined influence of sociodemographic characteristics, medication adherence, and self-care behaviors on glycemic control within the primary healthcare setting. This lack of localized, up-to-date evidence creates a gap in understanding the true determinants of inadequate glycemic control in this population. Addressing this gap is essential for designing targeted, context-specific interventions that can enhance the effectiveness of diabetes management programs and reduce complications. Given the importance of achieving adequate glycemic control to prevent complications and enhance quality of life, identifying the prevalence and determinants of poor glycemic control in patients with T2DM is essential. This cross-sectional study investigates these factors among patients attending comprehensive health centers in Qaemshahr, providing evidence to inform targeted interventions and healthcare planning.
Materials and Methods
Study design and setting
This cross-sectional analytical study was conducted in 2023 among patients with T2DM attending selected comprehensive health centers in Qaemshahr, Iran. A multistage sampling method was employed to select participants. During the study period, the researcher visited one selected health center each day and recruited eligible patients who attended for routine diabetes check-ups. In the study by Motamedi et al., the frequency of uncontrolled diabetes in the patients studied was 45.3% [8].
Sample size calculation
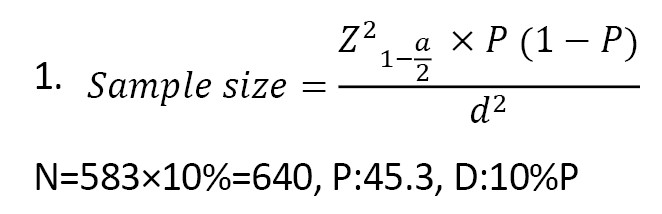
The sample size in the current study was 583 diabetics, calculated using the Equation 1. Therefore, the sample size was calculated at 640, accounting for the dropout rate, which was distributed according to the centers’ proportions, and random sampling was performed within each center separately, given that the number of diabetic patients in Qaemshahr was 24094 in 2023.
Multistage sampling will be used, with a combination of methods applied. Based on the results of the 2012 population census, categorized by urban and rural centers in Qaemshahr County, 5 selected population clusters were identified. For each center, the sample size was determined according to its population using the Equation 2:
2. nh=(nh/N)×n
1. North—Urban center No. 3: 92; 2. North—Chamazketi rural center: 48; 3. South—Vaskas rural center: 27; 4. South—Urban center No. 1: 154; 5. East—Sarukola rural center: 26; 6. East—Urban center No. 2: 190; 7. West—Joneid rural center: 26; 8. West—Urban center No. 5: 78.
Inclusion and exclusion criteria
A total of 642 patients with confirmed T2DM who met the inclusion criteria participated in the study. Inclusion criteria included being diagnosed with type 2 diabetes, willingness to participate, at least 1 year having passed since the person’s diabetes diagnosis, and being aged 30 to 80 years, and having recent laboratory data on fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c). Exclusion criteria included corticosteroid use, severe depression, pregnancy, and type 1 diabetes.
Data collection instruments
Data were collected using a structured questionnaire that included demographic information, clinical characteristics, and validated scales assessing diabetes self-care behaviors and medication adherence. The diabetes self-care questionnaire and the Morisky [9] medication adherence scale (MMAS-8) were administered to evaluate patients’ self-care and adherence, respectively. The diabetes self-care questionnaire by Toobert et al. [10] has been used in various studies [9, 10]. The content validity of the questionnaire was evaluated by 8 faculty experts using the content validity index (CVI), yielding an average score of 84.9%.
Moriski et al. [9] reported a Cronbach α coefficient of 0.83 for the MMAS-8. Also, in the study by Mehtak et al. [11] in 2018, MMAS-8 reliability was reported as 0.68 using the Cronbach α method, and the face and content validity were reported and confirmed [9, 11].
The reliability of the diabetes self-care questionnaire has been confirmed in various studies using the internal consistency method, with a Cronbach α coefficient of 0.78 [8, 12].
Definition of glycemic control
Glycemic control status was determined using the most recent FBG and HbA1c results, reflecting the patient’s glycemic status over the preceding 3 months. Patients were classified into two groups: Controlled glycemia, defined as FBG ≤130 mg/dL and HbA1c <7%, and uncontrolled glycemia, defined as FBG >130 mg/dL and/or HbA1c ≥7%.
Statistical analysis
Data analysis was performed using SPSS software, version 19. Descriptive statistics were used to summarize the sample characteristics. Inferential statistics, including the chi-square test and correlation analyses, were applied to examine the relationships between glycemic control and various demographic, clinical, and behavioral factors. Statistical significance was set at P<0.05 for all tests. Binary logistic regression analysis was used to determine factors associated with poor glycemic control. Glycemic control status (controlled vs uncontrolled) was treated as the dependent variable. Independent variables included demographic characteristics, clinical variables, medication adherence, and self-care behaviors. Variables with P<0.20 in univariate analyses were entered into the multivariable model. Model significance was assessed at P<0.05.
Ethical considerations
Ethical approval for the study was obtained from the relevant institutional review board, and informed consent was secured from all participants before data collection.
Results
A total of 642 patients with T2DM participated in the study. The demographic and clinical characteristics of the participants are presented in Table 1.
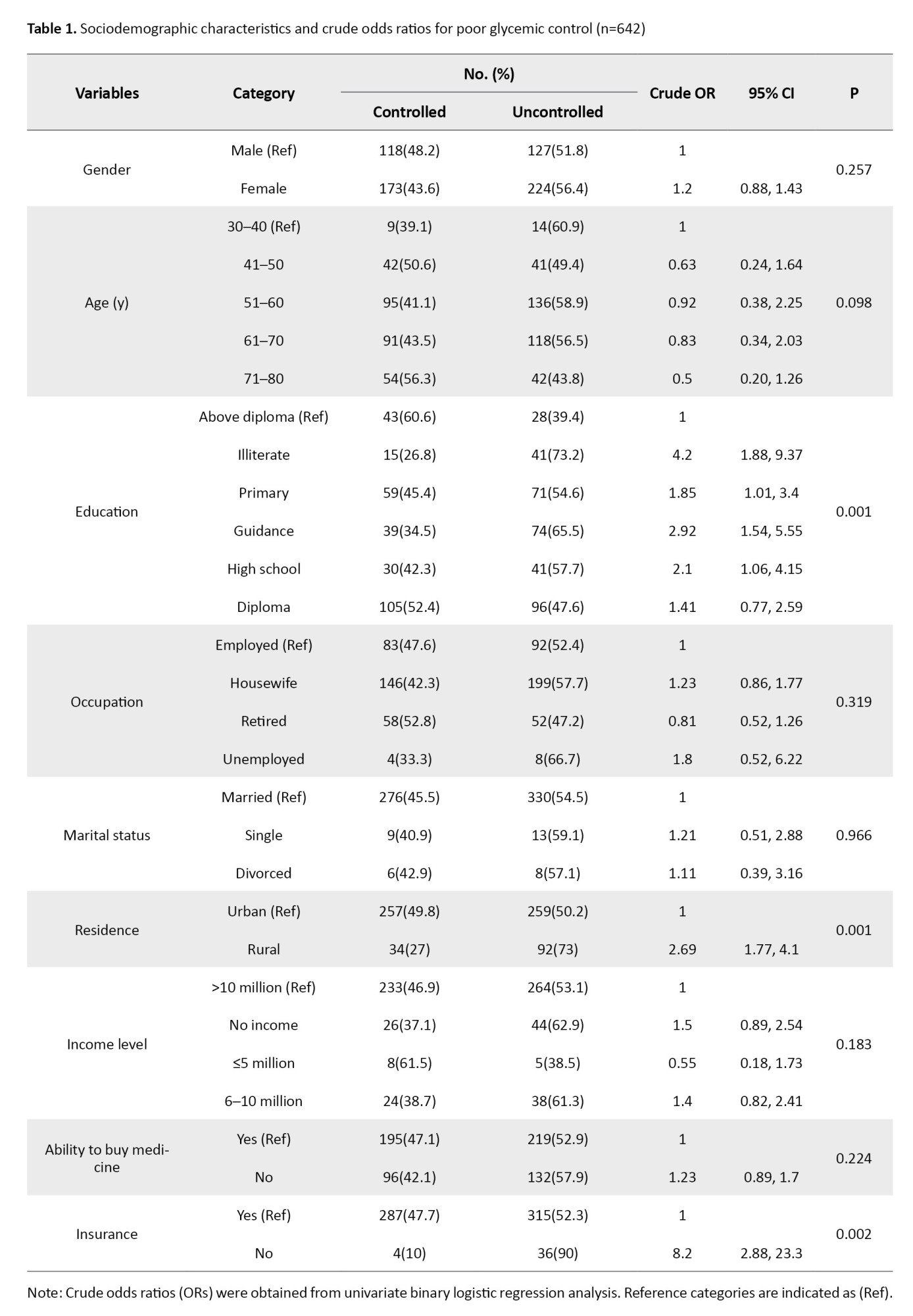
The prevalence of poor glycemic control was 45.3%. The prevalence of poor glycemic control (HbA1c ≥7%) among the participants was 54.7%, highlighting the ongoing challenges in diabetes management.
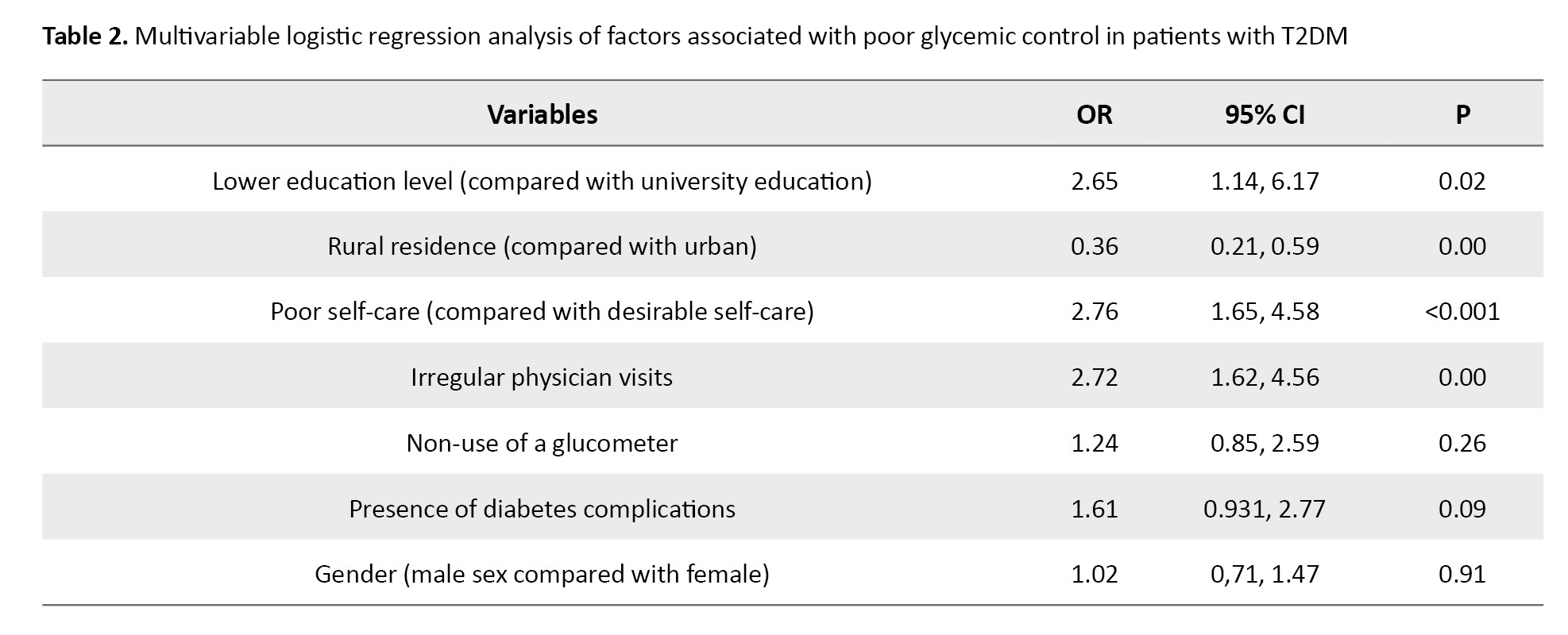
Statistically significant associations were found between glycemic control and several key factors, including patients’ education level, place of residence, type of health insurance, medication regimen, use of glucometer, regular physician visits, and regular visits to healthcare providers (P<0.05). However, no significant relationship was observed between glycemic control and gender, age, or marital status (P>0.05). According to logistic regression analysis, patients with lower levels of education had significantly higher odds of poor glycemic control (OR=2.65; 95% CI, 1.14%, 6.17%). Similarly, poor self-care was associated with increased odds of uncontrolled glycemia (OR=2.76; 95% CI, 1.65%, 4.58%) (Table 2).
Approximately 30.2% of patients demonstrated high medication adherence, which is promising; however, only 8.1% exhibited optimal self-care practices, including proper diet, regular exercise, and consistent blood glucose monitoring. This finding highlights the need for comprehensive diabetes education addressing all aspects of self-care, as medication adherence alone may not be sufficient to achieve glycemic targets. A significant association was observed between self-care behaviors and HbA1c levels (χ² test, P=0.001), indicating that better self-care is associated with improved glycemic control (Table 3).
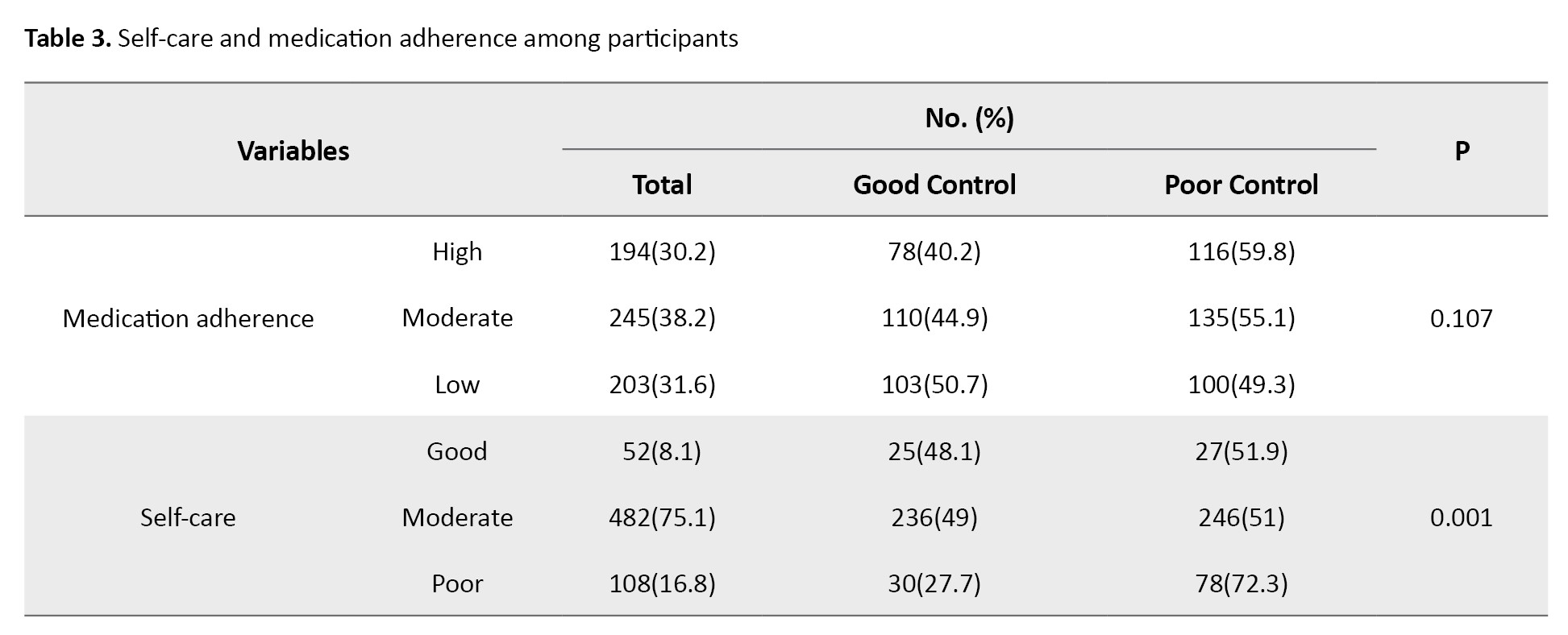
This result reinforces the importance of self-management in diabetes care.
Further analysis revealed significant relationships between self-care and factors such as frequency of physician and healthcare provider visits, presence of diabetes-related complications, ability to afford medications, household size, and living with family members (P<0.05) (Table 4).
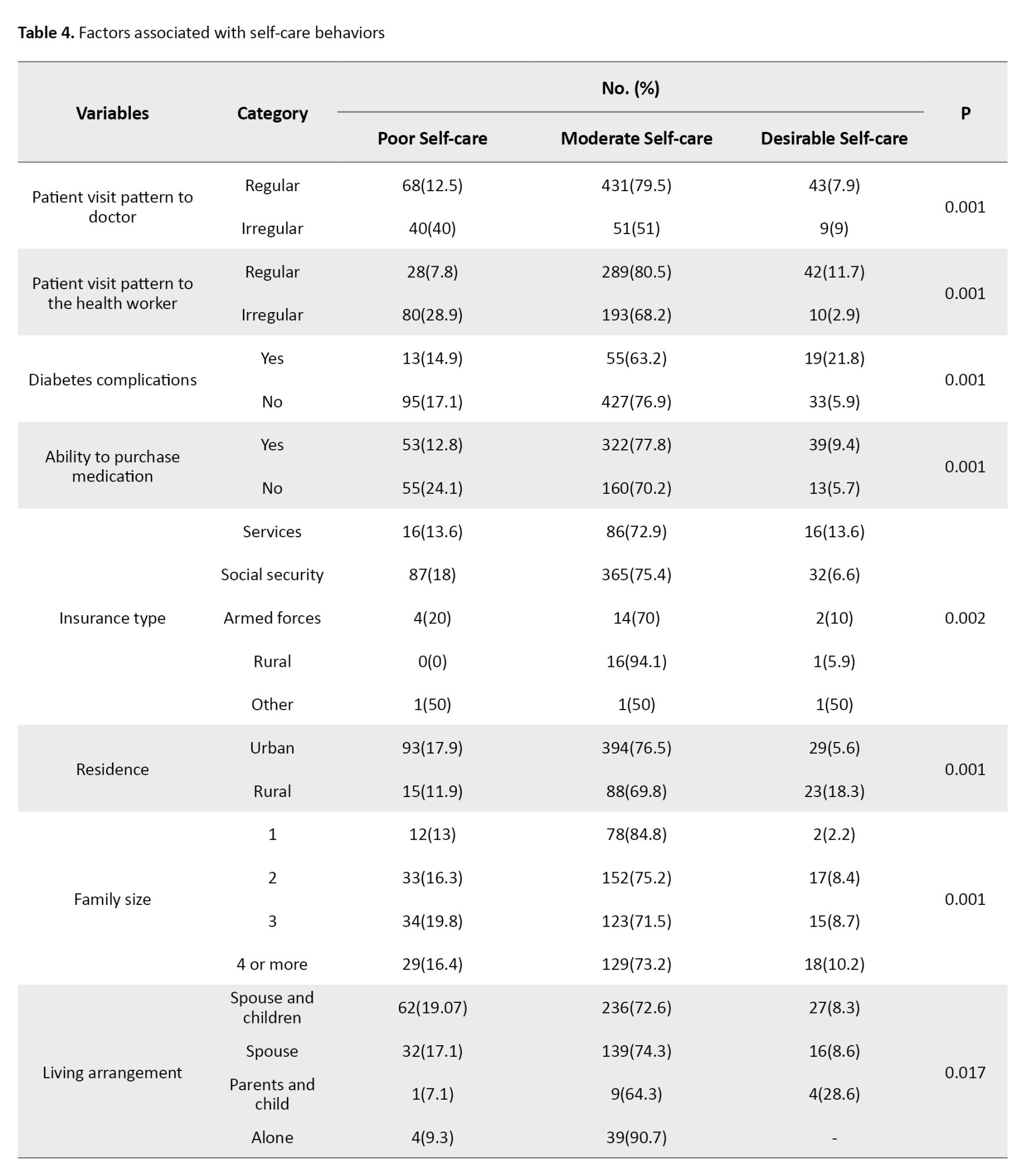
Poor self-care was strongly associated with uncontrolled glycemia (OR=2.76; 95% CI, 1.65%, 4.58%). These findings suggest that both regular healthcare engagement and sufficient financial resources for treatment are crucial for optimal self-care. Moreover, living with family members, which can provide emotional and practical support, was positively associated with self-care behaviors, highlighting the importance of social support. Interventions aimed at enhancing social support and reducing financial barriers should be considered integral components of diabetes management programs.
Interestingly, body mass index (BMI) and performance of foot care activities were significantly associated with HbA1c levels (P<0.05). This finding underscores the need for comprehensive diabetes management that goes beyond glucose monitoring, highlighting the interconnectedness of physical health—such as weight management and prevention of diabetic foot complications—with overall glycemic control. These findings suggest that interventions focusing on weight management and regular foot care screening should be considered essential components of comprehensive diabetes care to improve outcomes for patients with type 2 diabetes.
The presence of diabetes complications and the frequency of physician and healthcare visits were significantly correlated with self-care status (P=0.01). These results emphasize that managing existing complications and ensuring regular engagement with healthcare professionals are vital for enhancing self-care and improving glycemic outcomes. Highlighting the low rate of optimal self-care despite medication adherence underscores the clinical importance of implementing strategies that promote comprehensive self-care behaviors. Furthermore, patients with a longer duration of diabetes were more likely to have uncontrolled blood sugar levels.
Discussion
The results of the present study showed that 75% of participants had a moderate level of self-care. The diabetes self-care questionnaire by Toobert et al. [10] scores ranged from 34 to 67, with higher scores indicating better self-care. In this study, the scores were categorized to provide specific ranges for poor (34–45), average (46–55), and good (56–67) self-care if available. Similar findings have been reported in previous studies; for instance, Firouz in Mashhad found that 47% of individuals had poor self-care [13], while Dagnew et al. [14], Gholamzadeh Nikjoo et al. [15], and Maleka et al. also reported moderate levels of self-care among patients with type 2 diabetes [16]. These results highlight the need for targeted interventions to improve self-care behaviors in this population.
A significant relationship was observed between self-care and HbA1c levels in the present study. However, this correlation does not imply causation, as the cross-sectional design limits causal inferences. Although some studies, such as Maleka et al. in Gorgan, did not report a significant correlation, differences in study populations, such as the proportion of women, rural residency, and socioeconomic status, may explain these discrepancies [16]. These population characteristics may influence self-care behaviors and glycemic control by affecting access to healthcare, adherence to treatment, and overall patient engagement. Additionally, regular laboratory testing was significantly associated with HbA1c levels (P=0.001), emphasizing the importance of consistent monitoring and patient education.
No significant association between gender and self-care was found in the present study, which aligns with the reports by Hamadzadeh et al. [17] and Maleka et al. [16]. Descriptive statistics show that 33.8% of participants were unemployed with minimal income, 86.2% of whom were women, and 24% could not afford medications, highlighting potential gender-related disparities in financial capacity. Some studies have reported gender differences in self-care, suggesting that socioeconomic factors and financial resources may influence self-care behaviors. These findings indicate that interventions aiming to improve self-care should consider targeted support for individuals with lower financial capacity, particularly women.
Education level, age, and disease duration were also associated with self-care. Individuals with longer disease duration demonstrated higher self-efficacy in diet, exercise, glucose monitoring, and medication adherence, and consequently had lower HbA1c levels. These results underscore the importance of comprehensive diabetes education and strategies to enhance patient self-efficacy to improve glycemic control [18, 19].
BMI and foot care practices were significantly associated with HbA1c and self-care behaviors. The presence of diabetes-related complications was also related to lower levels of self-care, suggesting that poor adherence to preventive behaviors may lead to adverse outcomes [20]. These findings highlight specific clinical implications, including the need for targeted interventions to improve foot care and promote weight management among patients with type 2 diabetes.
Although income and employment were not directly associated with self-care, the ability to afford medications was significantly linked to self-care behaviors. This finding underscores the importance of supportive policies and interventions to reduce financial barriers to diabetes management.
Overall, this study’s findings indicate that comprehensive diabetes education, social support, financial assistance, regular monitoring, and management of complications are essential components for improving self-care behaviors and glycemic control in patients with type 2 diabetes. We suggest better income categorization or socioeconomic measurements in future research.
Conclusion
Improving self-care practices alongside medication adherence is crucial for effective management of type 2 diabetes. The present study’s findings, consistent with several previous reports, emphasize the importance of patient education and regular follow-up to maintain glycemic control and reduce complications. Discrepancies observed across studies may be explained by differences in population characteristics, such as gender distribution, socioeconomic status, and rural versus urban residence, underscoring the need to tailor interventions to specific patient groups.
Study limitations
The participation of men in this study was very low, which may limit the generalizability of the findings to male patients. Additionally, the study was cross-sectional, conducted over a short period, and limited to a specific geographical area, preventing any causal inferences. These limitations should be considered when interpreting the results, as they may introduce potential biases and affect the applicability of the findings to broader populations.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.IMAMHOSPITAL.REC.1402.101), and informed consent was secured from all participants before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Study design: Maryam Zarrinkamar; Methodology: Mohammad Khademloo; Data collection and investigation: Elham Alinejad; Data analysis: Roghaye Khatoon Arab and Mohammad Khademloo; Writing the original draft: Pejman Khosravi; Review, editing, and visualization: Mojgan Geran; Final approval: All authors.
Conflict of interest
The authors declared no Conflict of interest.
Acknowledgements
Thanks to the staff of the Qaemshahr County Health Network and the managers and staff of the comprehensive health centers mentioned in the study.
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Three out of every 4 people with diabetes (79%) live in low- and middle-income countries. Diabetes is the seventh leading cause of death in the United States and is consistently among the top 10 causes of death in Iran [1]. In Iran, the prevalence of T2DM is 9.6%, and about 5 million adults with diabetes live in the country. Iran is one of the countries in the region with the highest number of people with diabetes, and it is predicted that this number will double by 2045 [2].
The prevalence data is slightly outdated (estimates indicate that over 135 million adults worldwide were affected in 1993, a number projected to reach 300 million by 2025 [1].
Despite advances in treatment, glycemic control remains suboptimal in a significant proportion of patients, leading to increased risk of acute and chronic complications such as cardiovascular disease, nephropathy, neuropathy, and retinopathy. Between 40% and 60% of patients worldwide have poorly controlled diabetes. Although blood glucose control is the main goal of treatment, it is not achieved in most patients [2, 3].
A complex interplay of factors, including genetic predisposition, environmental conditions, lifestyle, socioeconomic status, and patient adherence to treatment regimens, influences poor glycemic control. Studies have identified age, gender, duration of diabetes, BMI, educational level, and family history as important contributors to glycemic outcomes [4, 5].
Moreover, self-care behaviors, encompassing medication adherence, dietary management, physical activity, and regular monitoring, are critical determinants of successful diabetes management [6]. However, research indicates that, despite a considerable proportion of patients demonstrating medication adherence, actual self-care practices remain inadequate, highlighting a gap in comprehensive diabetes management education and support [7]. This gap is of particular concern in low- and middle-income settings, where healthcare resources are limited, and the burden of diabetes complications is rising.
Despite extensive global and national efforts to improve diabetes management, glycemic control remains suboptimal in a substantial proportion of patients, particularly in low- and middle-income countries. Although numerous studies have examined predictors of poor glycemic control, most available evidence is either outdated, limited to specific subgroups, or lacks a comprehensive assessment of both medication adherence and self-care behaviors simultaneously. Moreover, the majority of regional studies in Iran have focused on hospital-based populations, with limited data available from primary care and community health centers where most patients with type 2 diabetes routinely receive care. In Qaemshahr City, Iran, despite the high and growing burden of diabetes, no recent study has systematically evaluated the combined influence of sociodemographic characteristics, medication adherence, and self-care behaviors on glycemic control within the primary healthcare setting. This lack of localized, up-to-date evidence creates a gap in understanding the true determinants of inadequate glycemic control in this population. Addressing this gap is essential for designing targeted, context-specific interventions that can enhance the effectiveness of diabetes management programs and reduce complications. Given the importance of achieving adequate glycemic control to prevent complications and enhance quality of life, identifying the prevalence and determinants of poor glycemic control in patients with T2DM is essential. This cross-sectional study investigates these factors among patients attending comprehensive health centers in Qaemshahr, providing evidence to inform targeted interventions and healthcare planning.
Materials and Methods
Study design and setting
This cross-sectional analytical study was conducted in 2023 among patients with T2DM attending selected comprehensive health centers in Qaemshahr, Iran. A multistage sampling method was employed to select participants. During the study period, the researcher visited one selected health center each day and recruited eligible patients who attended for routine diabetes check-ups. In the study by Motamedi et al., the frequency of uncontrolled diabetes in the patients studied was 45.3% [8].
Sample size calculation
The sample size in the current study was 583 diabetics, calculated using the Equation 1. Therefore, the sample size was calculated at 640, accounting for the dropout rate, which was distributed according to the centers’ proportions, and random sampling was performed within each center separately, given that the number of diabetic patients in Qaemshahr was 24094 in 2023.
Multistage sampling will be used, with a combination of methods applied. Based on the results of the 2012 population census, categorized by urban and rural centers in Qaemshahr County, 5 selected population clusters were identified. For each center, the sample size was determined according to its population using the Equation 2:
2. nh=(nh/N)×n
1. North—Urban center No. 3: 92; 2. North—Chamazketi rural center: 48; 3. South—Vaskas rural center: 27; 4. South—Urban center No. 1: 154; 5. East—Sarukola rural center: 26; 6. East—Urban center No. 2: 190; 7. West—Joneid rural center: 26; 8. West—Urban center No. 5: 78.
Inclusion and exclusion criteria
A total of 642 patients with confirmed T2DM who met the inclusion criteria participated in the study. Inclusion criteria included being diagnosed with type 2 diabetes, willingness to participate, at least 1 year having passed since the person’s diabetes diagnosis, and being aged 30 to 80 years, and having recent laboratory data on fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c). Exclusion criteria included corticosteroid use, severe depression, pregnancy, and type 1 diabetes.
Data collection instruments
Data were collected using a structured questionnaire that included demographic information, clinical characteristics, and validated scales assessing diabetes self-care behaviors and medication adherence. The diabetes self-care questionnaire and the Morisky [9] medication adherence scale (MMAS-8) were administered to evaluate patients’ self-care and adherence, respectively. The diabetes self-care questionnaire by Toobert et al. [10] has been used in various studies [9, 10]. The content validity of the questionnaire was evaluated by 8 faculty experts using the content validity index (CVI), yielding an average score of 84.9%.
Moriski et al. [9] reported a Cronbach α coefficient of 0.83 for the MMAS-8. Also, in the study by Mehtak et al. [11] in 2018, MMAS-8 reliability was reported as 0.68 using the Cronbach α method, and the face and content validity were reported and confirmed [9, 11].
The reliability of the diabetes self-care questionnaire has been confirmed in various studies using the internal consistency method, with a Cronbach α coefficient of 0.78 [8, 12].
Definition of glycemic control
Glycemic control status was determined using the most recent FBG and HbA1c results, reflecting the patient’s glycemic status over the preceding 3 months. Patients were classified into two groups: Controlled glycemia, defined as FBG ≤130 mg/dL and HbA1c <7%, and uncontrolled glycemia, defined as FBG >130 mg/dL and/or HbA1c ≥7%.
Statistical analysis
Data analysis was performed using SPSS software, version 19. Descriptive statistics were used to summarize the sample characteristics. Inferential statistics, including the chi-square test and correlation analyses, were applied to examine the relationships between glycemic control and various demographic, clinical, and behavioral factors. Statistical significance was set at P<0.05 for all tests. Binary logistic regression analysis was used to determine factors associated with poor glycemic control. Glycemic control status (controlled vs uncontrolled) was treated as the dependent variable. Independent variables included demographic characteristics, clinical variables, medication adherence, and self-care behaviors. Variables with P<0.20 in univariate analyses were entered into the multivariable model. Model significance was assessed at P<0.05.
Ethical considerations
Ethical approval for the study was obtained from the relevant institutional review board, and informed consent was secured from all participants before data collection.
Results
A total of 642 patients with T2DM participated in the study. The demographic and clinical characteristics of the participants are presented in Table 1.
The prevalence of poor glycemic control was 45.3%. The prevalence of poor glycemic control (HbA1c ≥7%) among the participants was 54.7%, highlighting the ongoing challenges in diabetes management.
Statistically significant associations were found between glycemic control and several key factors, including patients’ education level, place of residence, type of health insurance, medication regimen, use of glucometer, regular physician visits, and regular visits to healthcare providers (P<0.05). However, no significant relationship was observed between glycemic control and gender, age, or marital status (P>0.05). According to logistic regression analysis, patients with lower levels of education had significantly higher odds of poor glycemic control (OR=2.65; 95% CI, 1.14%, 6.17%). Similarly, poor self-care was associated with increased odds of uncontrolled glycemia (OR=2.76; 95% CI, 1.65%, 4.58%) (Table 2).
Approximately 30.2% of patients demonstrated high medication adherence, which is promising; however, only 8.1% exhibited optimal self-care practices, including proper diet, regular exercise, and consistent blood glucose monitoring. This finding highlights the need for comprehensive diabetes education addressing all aspects of self-care, as medication adherence alone may not be sufficient to achieve glycemic targets. A significant association was observed between self-care behaviors and HbA1c levels (χ² test, P=0.001), indicating that better self-care is associated with improved glycemic control (Table 3).
This result reinforces the importance of self-management in diabetes care.
Further analysis revealed significant relationships between self-care and factors such as frequency of physician and healthcare provider visits, presence of diabetes-related complications, ability to afford medications, household size, and living with family members (P<0.05) (Table 4).
Poor self-care was strongly associated with uncontrolled glycemia (OR=2.76; 95% CI, 1.65%, 4.58%). These findings suggest that both regular healthcare engagement and sufficient financial resources for treatment are crucial for optimal self-care. Moreover, living with family members, which can provide emotional and practical support, was positively associated with self-care behaviors, highlighting the importance of social support. Interventions aimed at enhancing social support and reducing financial barriers should be considered integral components of diabetes management programs.
Interestingly, body mass index (BMI) and performance of foot care activities were significantly associated with HbA1c levels (P<0.05). This finding underscores the need for comprehensive diabetes management that goes beyond glucose monitoring, highlighting the interconnectedness of physical health—such as weight management and prevention of diabetic foot complications—with overall glycemic control. These findings suggest that interventions focusing on weight management and regular foot care screening should be considered essential components of comprehensive diabetes care to improve outcomes for patients with type 2 diabetes.
The presence of diabetes complications and the frequency of physician and healthcare visits were significantly correlated with self-care status (P=0.01). These results emphasize that managing existing complications and ensuring regular engagement with healthcare professionals are vital for enhancing self-care and improving glycemic outcomes. Highlighting the low rate of optimal self-care despite medication adherence underscores the clinical importance of implementing strategies that promote comprehensive self-care behaviors. Furthermore, patients with a longer duration of diabetes were more likely to have uncontrolled blood sugar levels.
Discussion
The results of the present study showed that 75% of participants had a moderate level of self-care. The diabetes self-care questionnaire by Toobert et al. [10] scores ranged from 34 to 67, with higher scores indicating better self-care. In this study, the scores were categorized to provide specific ranges for poor (34–45), average (46–55), and good (56–67) self-care if available. Similar findings have been reported in previous studies; for instance, Firouz in Mashhad found that 47% of individuals had poor self-care [13], while Dagnew et al. [14], Gholamzadeh Nikjoo et al. [15], and Maleka et al. also reported moderate levels of self-care among patients with type 2 diabetes [16]. These results highlight the need for targeted interventions to improve self-care behaviors in this population.
A significant relationship was observed between self-care and HbA1c levels in the present study. However, this correlation does not imply causation, as the cross-sectional design limits causal inferences. Although some studies, such as Maleka et al. in Gorgan, did not report a significant correlation, differences in study populations, such as the proportion of women, rural residency, and socioeconomic status, may explain these discrepancies [16]. These population characteristics may influence self-care behaviors and glycemic control by affecting access to healthcare, adherence to treatment, and overall patient engagement. Additionally, regular laboratory testing was significantly associated with HbA1c levels (P=0.001), emphasizing the importance of consistent monitoring and patient education.
No significant association between gender and self-care was found in the present study, which aligns with the reports by Hamadzadeh et al. [17] and Maleka et al. [16]. Descriptive statistics show that 33.8% of participants were unemployed with minimal income, 86.2% of whom were women, and 24% could not afford medications, highlighting potential gender-related disparities in financial capacity. Some studies have reported gender differences in self-care, suggesting that socioeconomic factors and financial resources may influence self-care behaviors. These findings indicate that interventions aiming to improve self-care should consider targeted support for individuals with lower financial capacity, particularly women.
Education level, age, and disease duration were also associated with self-care. Individuals with longer disease duration demonstrated higher self-efficacy in diet, exercise, glucose monitoring, and medication adherence, and consequently had lower HbA1c levels. These results underscore the importance of comprehensive diabetes education and strategies to enhance patient self-efficacy to improve glycemic control [18, 19].
BMI and foot care practices were significantly associated with HbA1c and self-care behaviors. The presence of diabetes-related complications was also related to lower levels of self-care, suggesting that poor adherence to preventive behaviors may lead to adverse outcomes [20]. These findings highlight specific clinical implications, including the need for targeted interventions to improve foot care and promote weight management among patients with type 2 diabetes.
Although income and employment were not directly associated with self-care, the ability to afford medications was significantly linked to self-care behaviors. This finding underscores the importance of supportive policies and interventions to reduce financial barriers to diabetes management.
Overall, this study’s findings indicate that comprehensive diabetes education, social support, financial assistance, regular monitoring, and management of complications are essential components for improving self-care behaviors and glycemic control in patients with type 2 diabetes. We suggest better income categorization or socioeconomic measurements in future research.
Conclusion
Improving self-care practices alongside medication adherence is crucial for effective management of type 2 diabetes. The present study’s findings, consistent with several previous reports, emphasize the importance of patient education and regular follow-up to maintain glycemic control and reduce complications. Discrepancies observed across studies may be explained by differences in population characteristics, such as gender distribution, socioeconomic status, and rural versus urban residence, underscoring the need to tailor interventions to specific patient groups.
Study limitations
The participation of men in this study was very low, which may limit the generalizability of the findings to male patients. Additionally, the study was cross-sectional, conducted over a short period, and limited to a specific geographical area, preventing any causal inferences. These limitations should be considered when interpreting the results, as they may introduce potential biases and affect the applicability of the findings to broader populations.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.IMAMHOSPITAL.REC.1402.101), and informed consent was secured from all participants before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Study design: Maryam Zarrinkamar; Methodology: Mohammad Khademloo; Data collection and investigation: Elham Alinejad; Data analysis: Roghaye Khatoon Arab and Mohammad Khademloo; Writing the original draft: Pejman Khosravi; Review, editing, and visualization: Mojgan Geran; Final approval: All authors.
Conflict of interest
The authors declared no Conflict of interest.
Acknowledgements
Thanks to the staff of the Qaemshahr County Health Network and the managers and staff of the comprehensive health centers mentioned in the study.
References
- Jafarvand E, Ataey A, Edalati S. Epidemiology and death trends due to diabetes in Iran. Internal Medicine Today. 2021; 27(2):198-213. [DOI:10.32598/hms.27.2.2764.1]
- Epakchipoor F, Bastani F, Pashaei Sabet F. Self-management and medication adherence in older adults with type II diabetes referring to endocrinology clinics affiliated to Iran University of Medical Sciences (2019). Iran Journal of Nursing. 2021; 34(129):1-14. [DOI:10.52547/ijn.34.129.1]
- Bahrami Taghanaki H, Mosa Farkhani E, Eftekhari Gol R, Bahrami Taghanaki P, Bokaei S, Taghipour A, et al. Determinants of diabetic complications: A population-based case-control study. Iranian Journal of Epidemiology. 2020; 16(3):220-29. [Link]
- Kayar Y, Ilhan A, Kayar NB, Unver N, Coban G, Ekinci I, et al. Relationship between poor glycemic control and risk factors, lifestyle and complications. Biomedical Research. 2017; 28(4):1581-86. [Link]
- ElSayed NA, Aleppo G, Bannuru RR, Bruemmer D, Collins BS, Ekhlaspour L, et al. Diagnosis and classification of diabetes: Standards of care in diabetes-2024. Diabetes Care. 2024; 47(Suppl 1). [DOI:10.2337/dc24-S002] [PMID]
- Sadeh Tabarian M, Ghyasvandian S, Haghani S. Effect of education based on illness perception on glycemic control in diabetic patients. Iranian Journal of Endocrinology and Metabolism. 2020; 21(6):364-71.
- Nascimento T, Andrade A, Pinto E, Cabrita C, Pais S, Puerta RDL. Medication adherence and glycemic control in older adults with type 2 diabetes: A cross-sectional study in a community setting. Diabetology. 2025; 6(5):33. [DOI:10.3390/diabetology6050033]
- Motamedi N, Ahmadi H, Sanei M. Prevalence of uncontrolled diabetes and its predictors in patients with type 2 diabetes covered by comprehensive health care centers of Isfahan. Iranian Journal of Endocrinology and Metabolism. 2022; 23(6):369-77. [Link]
- Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Retracted: Predictive validity of a medication adherence measure in an outpatient setting. Journal of Clinical Hypertension. 2008; 10(5):348-54. [DOI:10.1111/j.1751-7176.2008.07572.x] [PMID]
- Toobert DJ, Glasgow RE, Acuna JD. (1997). The language of diabetes: Lay definitions of the social context of diabetes self-management. Diabetes Care. 1997; 20(9 1417-21.
- Mehrtak M, Hemmati A, Bakhshzadeh A. [Health literacy and its relationship with medical, dietary adherence and exercise in patients with type II diabetes mellitus (Persian)]. Journal of Health Literacy. 2018; 3(2):137-44. [Link]
- Shayeghian Z, Amiri P, Aguilar-Vafaie ME, Besharat MA. Effectiveness of acceptance and commitment group therapy on improvement of glycated hemoglobin and self-care activities in patients with type II diabetes. Contemporary Psychology. 2016; 10(2):41-50. [Link]
- Firooz M, Hosseini SJ, Mazlom SR, Hasan Zadeh F, Kimiyaee SA. Self-care of patients with type II diabetes. Journal of Sabzevar University of Medical Sciences. 2016; 22(6):1018-25.
- Dagnew B, Debalkie Demissie G, Abebaw Angaw D. Systematic review and meta-analysis of good self-care practice among people living with type 2 diabetes mellitus in Ethiopia. Evidence-Based Complementary and Alternative Medicine. 2021; 2021:8896896. [DOI:10.1155/2021/8896896] [PMID]
- Gholamzadeh Nikjoo R, Mohseni M. Self-care ability of diabetic patients referring to Tabriz University of Medical Sciences clinics. Depiction of Health. 2019.
- Maleka A, Khosravi S, Charkazi A, Pahlavanzadeh B, Khosravi Z, Khosravi M. Relationship between self-care behaviors and glycosylated hemoglobin level in diabetic patients. Journal of Gorgan University of Medical Sciences. 2020; 22(4):84-91.
- Hamadzadeh S, Ezatti Z, Abedsaeidi Z, Nasiri N. [Coping styles and self-care behaviors among diabetic patients (Persian)]. Iran Journal of Nursing. 2013; 25(80):24-33.
- Parham M, Riahin A, Jandaghi M, Darivandpour A. Self-care behaviors of diabetic patients in Qom. 2012.
- Rezaei Z, Ghaderi N, Nouri E, Ahmadi MA, Ghaderi E, Shakiba N, et al. Self-care agency and associated factors in patients with type 2 diabetes referred to Tohid Hospital in Sanandaj in 2016. Journal of Health Field. 2019; 7(3):40-8.
- D’Souza MS, Karkada SN, Parahoo K, Venkatesaperumal R, Achora S, Cayaban ARR. Self-efficacy and self-care behaviours among adults with type 2 diabetes. Applied Nursing Research. 2017; 36:25-32. [DOI:10.1016/j.apnr.2017.05.004] [PMID]
Type of Study: Original Article |
Subject:
Health care Management
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
