

Volume 14, Issue 1 (Winter 2026)
Iran J Health Sci 2026, 14(1): 35-46 |
Back to browse issues page


Ethics code: IR.MAZUMS.REC.1403.480
Clinical trials code: not applicable
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Naseripoor S, Jorbonyan A, Moosazadeh M, Ilali E S. Association of Personality Traits and Self-efficacy With Caregiver Burden in Family Caregivers of Frail Elderly: A Cross-sectional Study. Iran J Health Sci 2026; 14 (1) :35-46
URL: http://jhs.mazums.ac.ir/article-1-1114-en.html
URL: http://jhs.mazums.ac.ir/article-1-1114-en.html



Department of Geriatric Health, School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran. , paradis2082000@yahoo.com
Full-Text [PDF 888 kb]
(126 Downloads)
| Abstract (HTML) (311 Views)
References
Full-Text: (69 Views)
Introduction
Aging is a natural and inevitable stage of life that is rapidly expanding due to increased life expectancy, declining birth rates, and socio-economic development [1]. This accelerating global aging trend is particularly significant, as it is accompanied by widespread geriatric syndromes that impose substantial healthcare and caregiving burdens on families and health systems [2, 3]. One of the most critical geriatric syndromes is frailty, characterized by decreased physiological resilience to stressors and associated with adverse outcomes, such as disability, functional decline, increased dependency, and reduced quality of life (QoL) [4, 5]. Its prevalence in community-dwelling older adults in Asian countries, based on the fried frailty phenotype, is estimated at 28.0% (95% confidence Interval [CI], 21.3%, 35.3%) [6].
Numerous studies have demonstrated considerable caregiver burden when caring for frail elderly individuals, arising from financial responsibilities, role changes, assistance with activities of daily living, and managing behavioral issues, which can lead to decreased mental health, increased anxiety, maladaptive coping strategies, and reduced quality of care for both caregivers and care recipients [7-9]. This burden can decrease mental health, increase anxiety, maladaptive coping strategies, reduce quality of care, and diminish QoL for both caregiver and care recipient [10, 11]. Despite the availability of formal care services, the primary caregiving role remains with informal family caregivers, who often provide care without formal training and at no cost [12]. Pesantes et al. found that about 95% of the caregiving burden for dependent and disabled individuals falls on family members [13]. This condition exposes family caregivers to diverse physical, emotional, financial, and social challenges [14]. Therefore, identifying factors associated with caregiver burden among family caregivers is crucial.
Research indicates that personal resources and coping abilities play a significant role in reducing caregiver burden [15, 16]. For example, personality traits influence how individuals respond to stress and behave in various situations [17]. Personality is defined as an organized, stable set of relatively enduring characteristics that distinguish individuals [18]. It affects information processing and resistance to opposing views, which are important for caregivers who must make difficult decisions or face conflicting information [19]. Caregivers with higher neuroticism report greater caregiver burden and health problems, while those with higher extraversion scores tend to have better physical and mental health [20, 21]. However, targeting personality traits alone may be limited in effectiveness because they are relatively stable after age 30, highlighting the need to explore other flexible resources that influence caregiver burden [22].
Self-efficacy, as defined by Bandura, refers to an individual’s belief in their capability to execute the actions necessary to manage prospective situations and exert control over events [23]. Higher self-efficacy is associated with greater persistence in the face of challenges, lower perceived stress, and more effective regulation of emotional states; it plays a particularly central role among caregivers, who frequently encounter challenging and unpredictable situations [24]. In this context, studies on family caregivers have demonstrated that greater self-efficacy is linked to improved QoL, enhanced psychological well-being, and better sleep quality among those caring for older adults with chronic illnesses and dementia [25, 26].
Given the strong preference of many older adults for aging in place, the role of family caregivers in contemporary healthcare systems has become increasingly prominent, and the resulting caregiver burden warrants special attention. In this regard, conducting targeted research to identify factors that effectively reduce caregiver burden and enhance care quality is essential, ultimately contributing to the preservation of older adults’ independence and health. A review of the research literature indicates that most studies on caregiver burden have focused on caregivers of individuals with specific diseases, such as dementia or cancer. In contrast, dedicated investigations into family caregivers of frail elderly, characterized by heightened sensitivity to relatively minor stressors, greater dependency, and elevated risks of hospitalization and mortality, remain highly limited, particularly in Iran. Furthermore, examining the roles of psychological factors, such as the big five personality traits and self-efficacy as a positive psychological resource, can provide deeper insights into the determinants of caregiver burden and pave the way for the development of person-centered, evidence-based educational and support interventions. Accordingly, the present study aimed to investigate the associations among self-efficacy, personality traits, and caregiver burden among family caregivers of frail elderly in Garmeh County, North Khorasan Province, Iran.
Materials and Methods
This cross-sectional analytical study was conducted on 243 family caregivers of frail elderly residing in Garmeh County, North Khorasan, Iran, during 2025 (April to June). The study population included all family caregivers of frail elderly living at home and visiting health centers in Garmeh County. The sample size was calculated using G*Power software, version 3.1 with the “exact-correlation: Bivariate normal model” option for a bivariate correlation test, employing an a priori analysis for a two-tailed test based on an effect size (Correlation ρ H1=0.22) from Yang et al. [27], α=0.05, power=0.90, and ρ H0=0, yielding 213 participants corresponding to this specific model. To account for potential non-response, the sample size was increased by 30 participants, bringing the total to 243. Frail elderly were identified from the integrated health care system (SIB) database of Garmeh County based on assessments of nutritional status, body mass index (BMI), mental health status, ability to perform daily activities, need for assistance in personal affairs, dependency status, and need for care.
Sampling was performed by a two-stage random method: First, clusters were selected using cluster sampling from 6 urban comprehensive health service centers and 4 rural health centers. Then, individuals were selected using random sampling (random number table). After obtaining necessary permissions and identifying frail elderly, caregivers (one per frail elderly) were contacted by phone, given verbal consent, and informed about the study objectives. Then, they were invited to participate in health centers. In the next stage, written informed consent was obtained from eligible participants, who were assured of confidentiality. Data collection tools were completed by the caregivers under the researcher’s supervision.
The inclusion criteria included aged 18 years or older, residence in Garmeh County, continuous caregiving for a frail elderly individual for at least the past 6 months, ability to communicate and fluency in Persian, informal caregiver status, no history of psychiatric disorders under treatment (such as schizophrenia, severe depression, cognitive disorders) based on self-report and medical records, and informed consent. The exclusion criterion was incomplete or partially completed questionnaires.
The data collection instruments
Demographic information form included variables such as age, gender, residential status, education level, employment status, income level, physical disease, psychiatric history, history of visits to psychiatrists, and experience of stressful events in the past 6 months.
The general self-efficacy scale (GSE-17) was developed by Sherer et al. in 1982. This scale consists of 17 items [28]. The scoring method is based on a 5-point Likert scale ranging from strongly agree=1 to strongly disagree=5, with a total score range from 17 to 85. Items 1, 3, 8, 9, 13, and 15 are scored directly, while others are reverse-scored. Scores between 17 and 34 indicate low self-efficacy, 34 to 51 moderate self-efficacy, and scores above 51 indicate high self-efficacy [29, 30]. Psychometric properties of the Persian version, including criterion and construct validity, were confirmed by Delavar et al., with a Cronbach α reliability coefficient of 0.79, which is acceptable [31].
The caregiver burden inventory (CBI) assessed caregiver burden using the 24-item version. CBI was developed by Novak and Guest [32]. The inventory consists of 5 subscales: Time-dependent burden (items 1-5), developmental burden (items 6-10), physical burden (items 11-14), social burden (items 15-19), and emotional burden (items 20-24). Responses are rated on a 5-point Likert scale from never (0) to almost always (4). Total scores range from 0 to 96; scores of 36 or higher indicate a high caregiver burden. Internal consistency for the subscales, as measured by Cronbach α in the original inventory, ranged from 0.79 to 0.93 [33]. Shafiezadeh et al. translated and validated the 24-item Persian version, reporting Cronbach α of 0.93 for the total scale and 0.70-0.89 for subscales [34]. In our sample, Cronbach α was 0.94 (total) and 0.89-0.92 (subscales).
The ten-item personality inventory (TIPI) assessed personality traits using Gosling et al.’s 10-item TIPI [35]. The 5 traits measured are extraversion (sociality, sociability), agreeableness (empathy, helpfulness), conscientiousness (orderliness, achievement striving), emotional stability (versus neuroticism), and openness to experience (curiosity, creativity). Each trait is measured with two items. The TIPI is popular due to its cost- and time-efficiency, and can be completed by individuals with minimal literacy. Responses are on a 7-point Likert scale ranging from strongly disagree to agree strongly. Total personality scores range from 10 to 70. Some items are reverse-scored. Gosling et al. [35] reported Cronbach α for subscales between 0.40 and 0.73 in a sample of 1813 participants. In Iran, Azkhosh et al. standardized and localized the scale in a sample of 160 elderly individuals (aged 66 to 71), reporting a Cronbach α of 0.51 for the overall scale and 0.40 to 0.60 for the subscales [36].
Data analysis
The collected data in this study were analyzed using SPSS software, version 26. Initially, the data were screened for outliers. Descriptive statistics, including frequency, percentage, Mean±SD, were used to describe the variables. Inferential statistical tests, including independent t-tests, analysis of variance (ANOVA), Pearson correlation coefficient, and multiple linear regression (simultaneous approach with variables selected based on univariate P<0.2), were employed to examine relationships among variables. The normality of data distribution was assessed using skewness and kurtosis tests. A significance level of less than or equal to 0.05 was considered for all statistical tests.
Results
A total of 243 participants were included in this study. The Mean±SD age of the participants (caregivers) was 51.6±11.3) years. Most participants were married (76.1%), and 90.5% were female. Regarding education, 16.5% of the participants were illiterate. Table 1 presents detailed demographic characteristics of the participants.
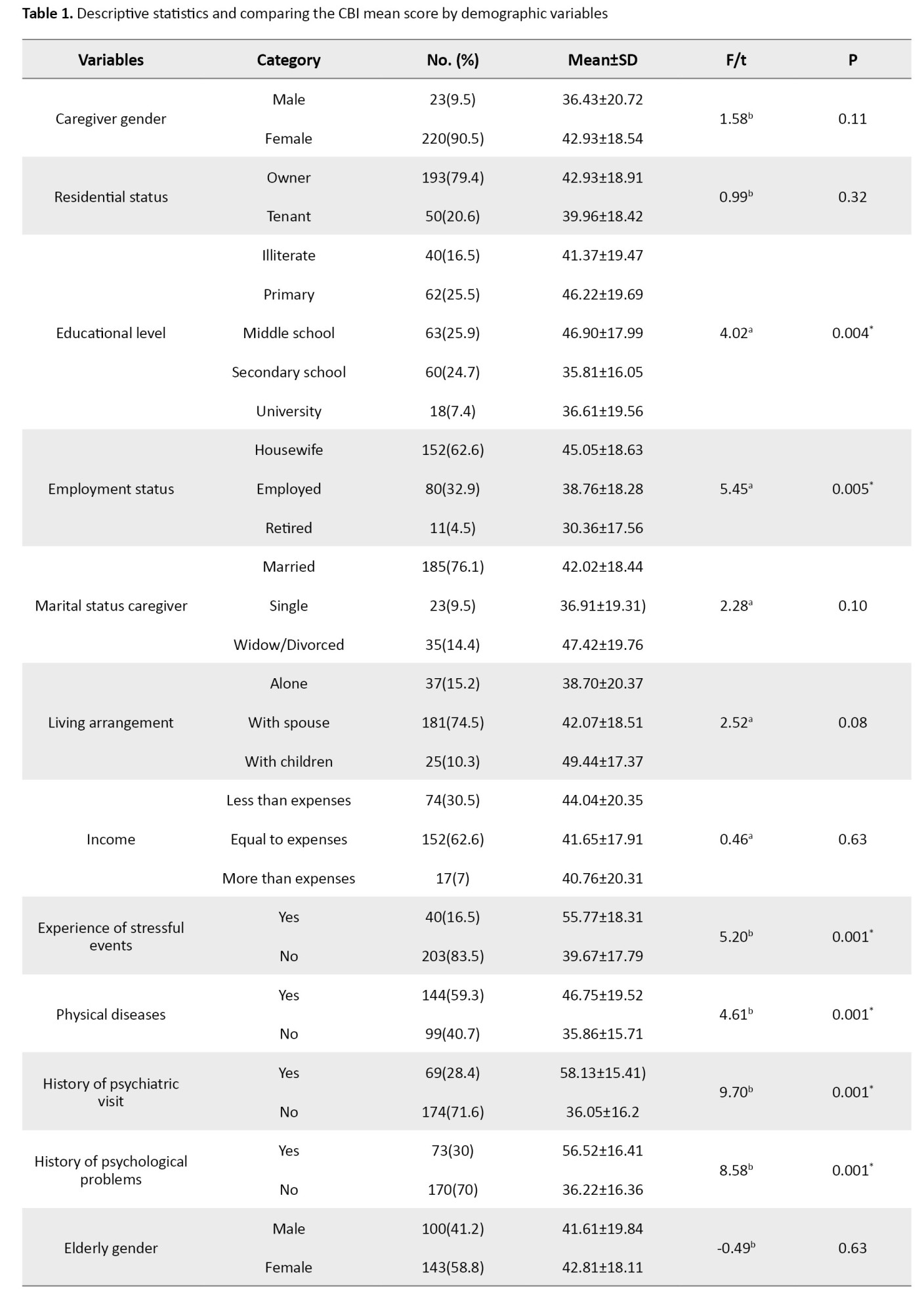
Independent t-test results showed that having physical diseases, a history of psychological problems, past psychiatric visits, and experiencing stressful events in the last 6 months were significantly associated with increased caregiver burden (P≤0.05). However, no significant association was found between caregiver burden and the gender of the caregiver or the older person, or residential status (P> 0.05) (Table 1).
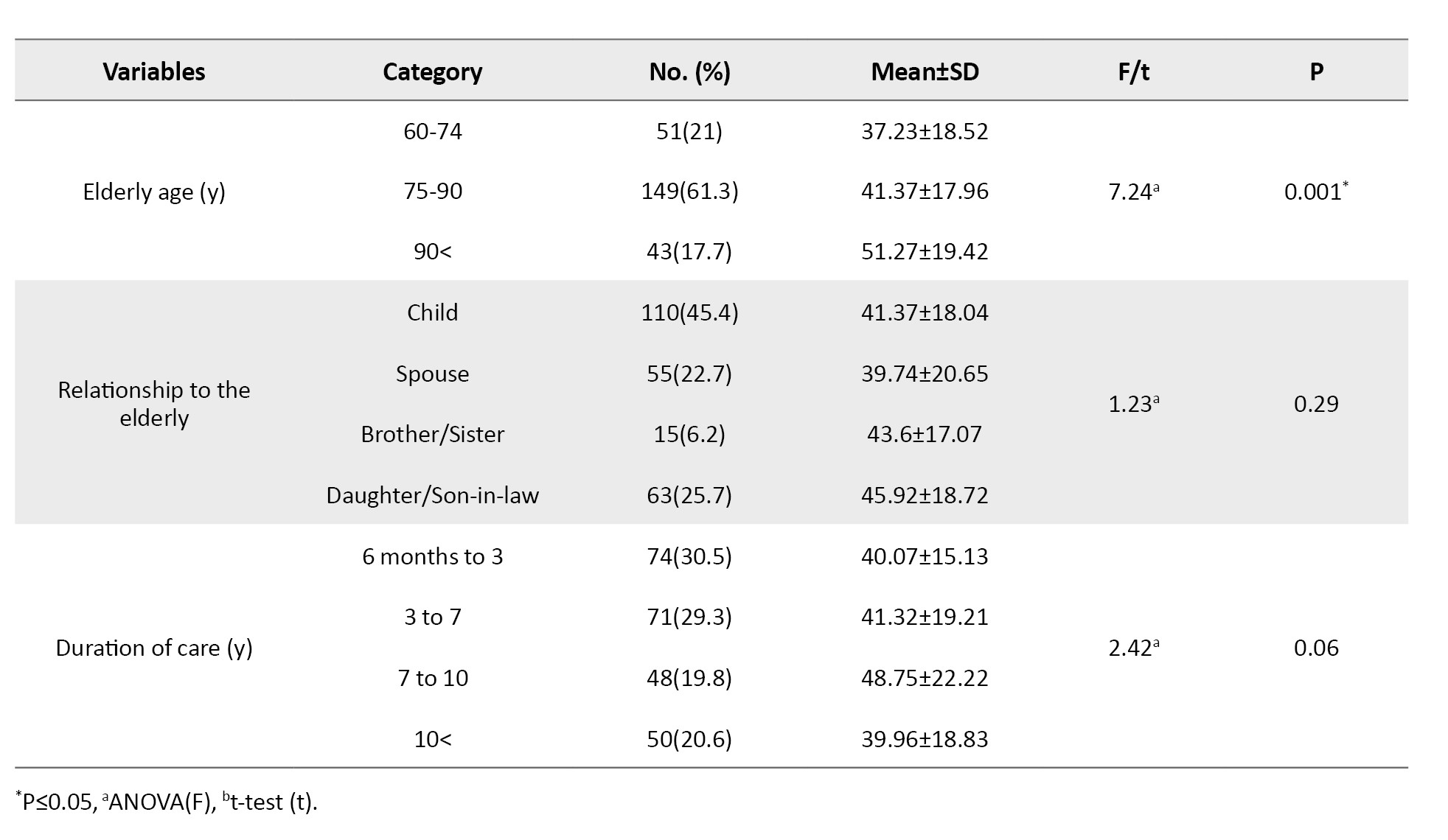
ANOVA revealed significant differences in mean caregiver burden scores across groups classified by caregivers’ education level, employment status, and the age group of the cared-for elderly (P≤0.05) (Table 1). Post-hoc Tukey tests revealed that caregivers of older people aged 60-74 years experienced significantly lower burden than those caring for those aged ≥85 years (P<0.01). University-educated caregivers reported lower burden than those with primary education (P<0.01). Homemakers had a higher burden than employed (P<0.01) and retired caregivers (P<0.05). No significant differences were found for caregiving duration, living arrangement, or relationship to older people (P>0.05) (Table 1).
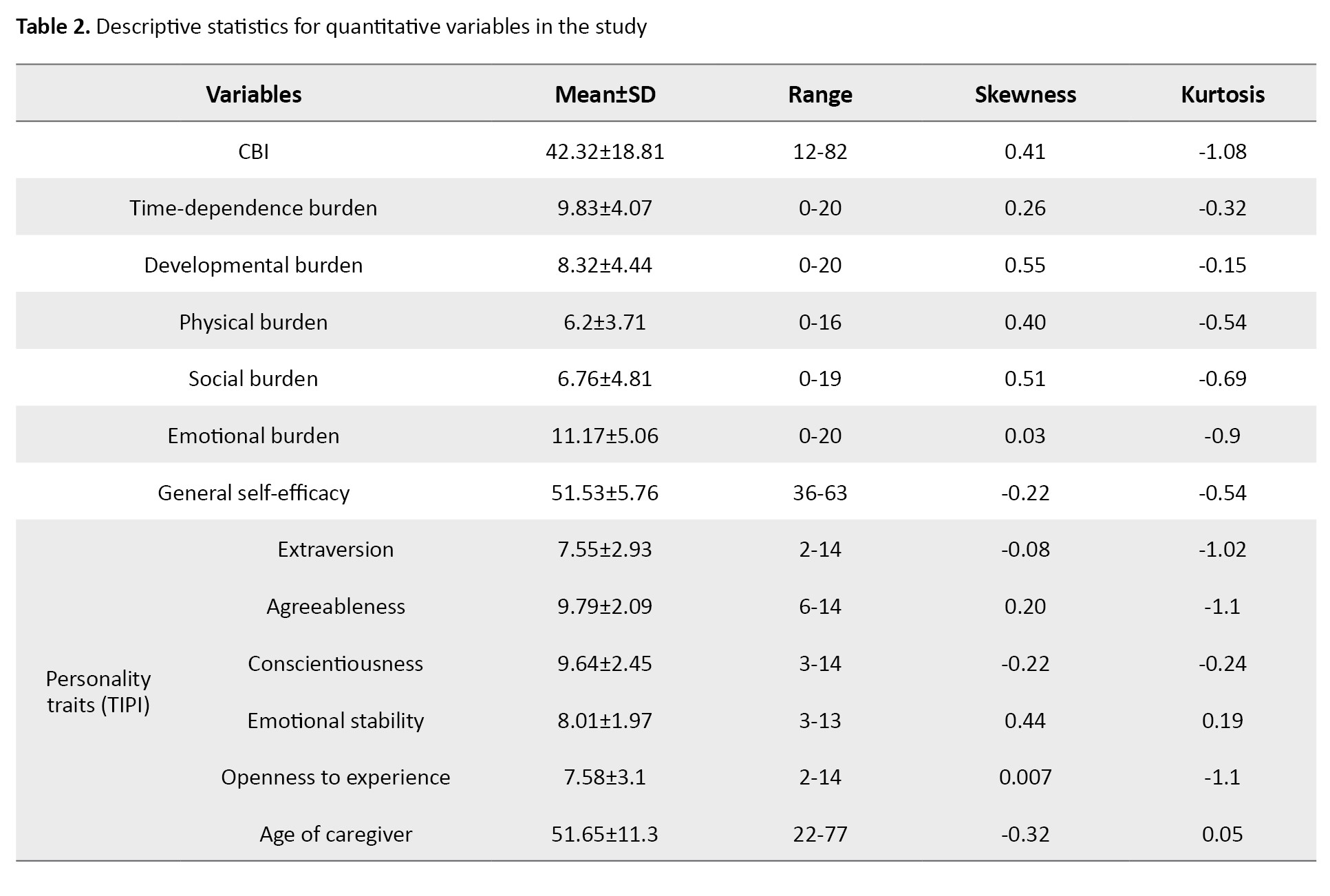
Normality test results based on skewness and kurtosis indicated that the data were within the acceptable range (-2 to +2), confirming normality. The Mean±SD score of the CBI was 42.32(18.81). Of 247 caregivers, 126(51%) had CBI scores ≥36, confirming substantial prevalence of high caregiver burden. Among the caregiver burden components, emotional burden had the highest Mean±SD score of 11.17(5.06). Descriptive statistics of the quantitative variables are presented in Table 2.
The correlation analysis results revealed a significant negative association between general self-efficacy and CBI in the present study (r=-0.56, P≤0.05). This finding indicates that as caregivers’ self-efficacy levels increase, their caregiver burden decreases. Among the caregiver burden subscales, emotional burden showed the strongest negative correlation with self-efficacy (r=-0.57, P≤0.001), whereas physical burden had the weakest correlation (r=-0.40, P<0.001) (Table 3).
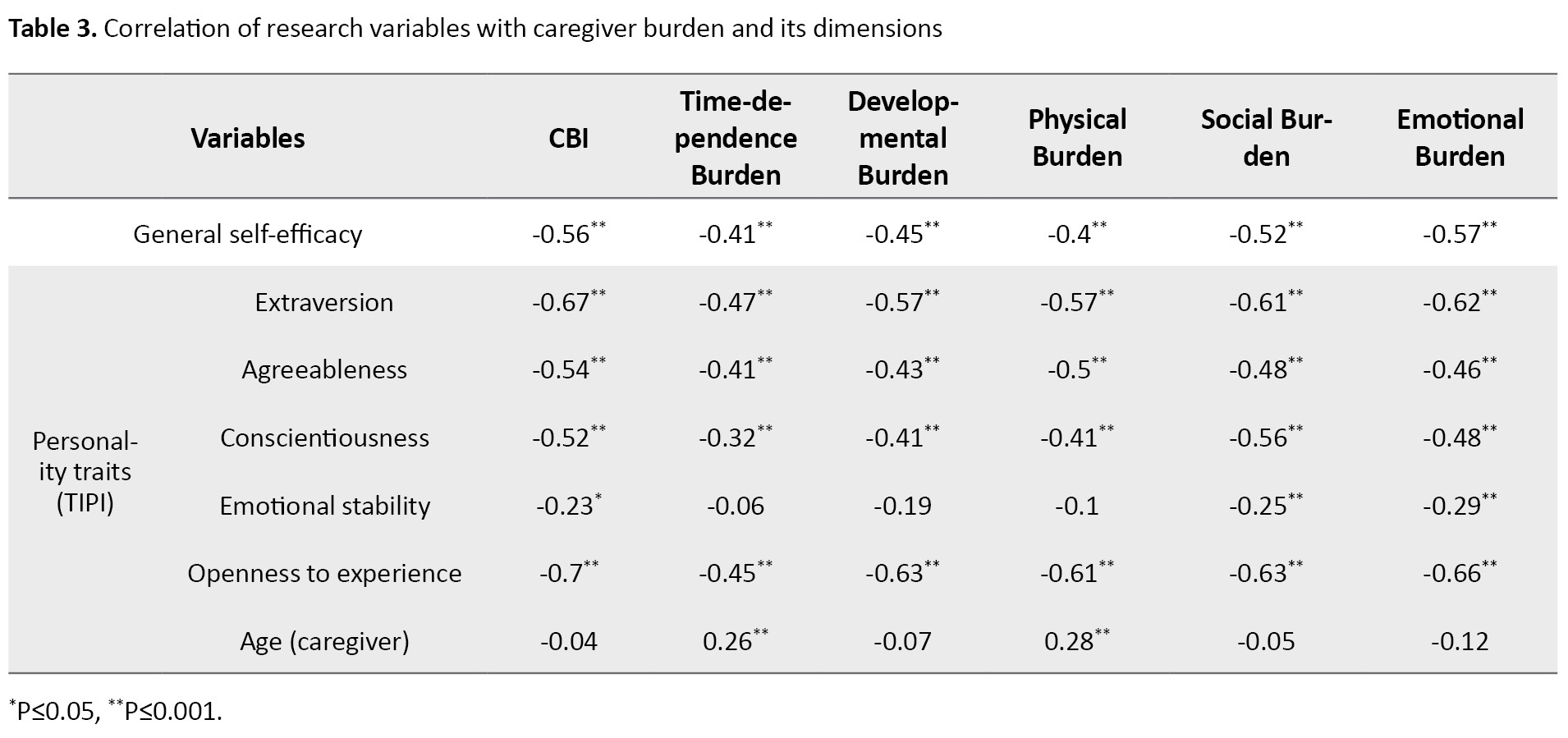
Additionally, caregiver burden was significantly and negatively correlated with personality traits (P≤0.05). Among these, extraversion (r=-0.67, P<0.05) and openness to experience (r=-0.70, P<0.05) had the strongest associations with caregiver burden. This finding suggests that individuals who are more extraverted and open to new experiences experience less caregiver burden. No significant association was found between caregiver age and overall CBI (P≥0.05); however, positive and significant correlations were observed between age and physical burden (r=0.28, P≤0.05) as well as time-dependent burden (r=0.26, P≤0.05) (Table 3).
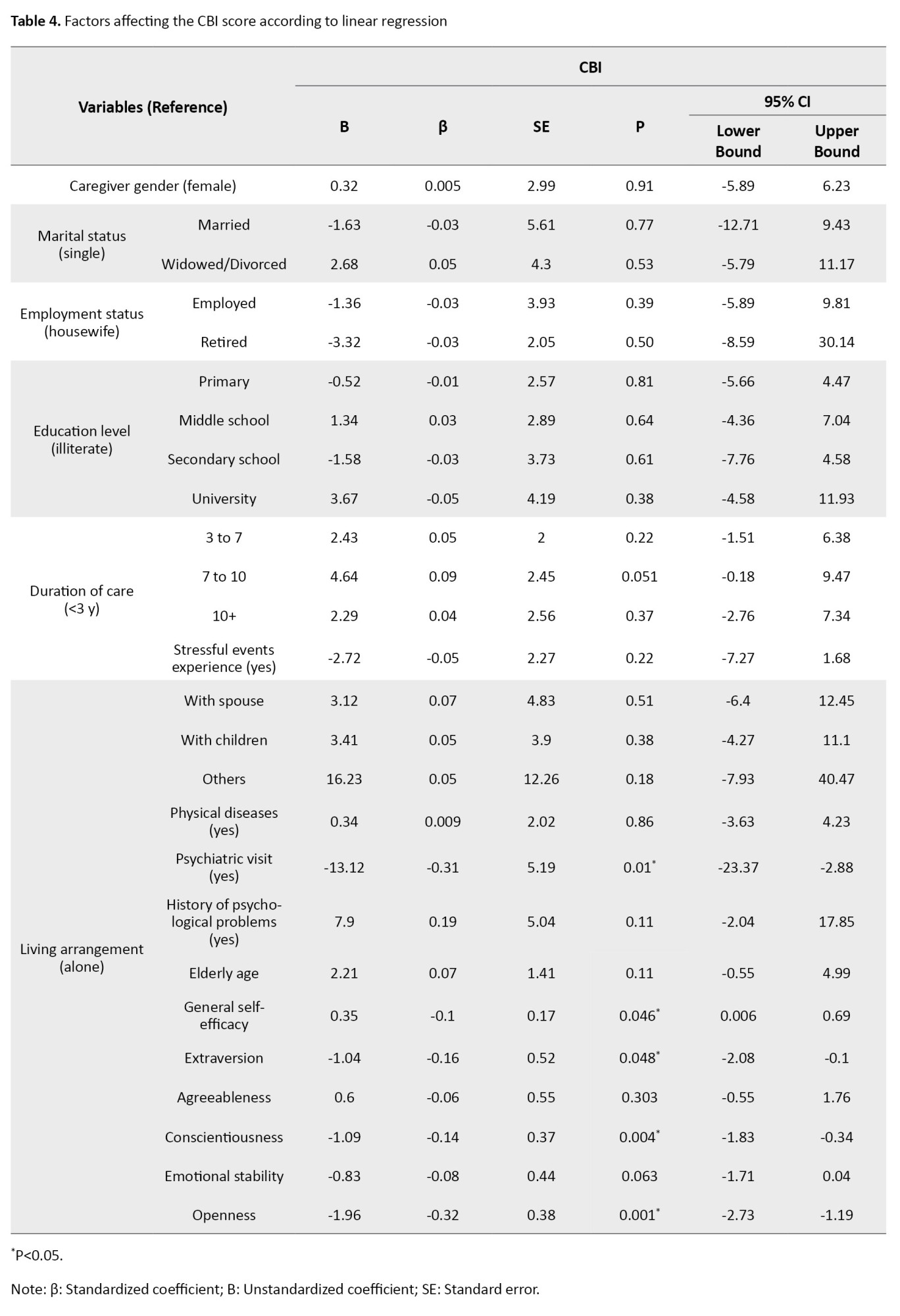
In this study, a simultaneous multiple regression analysis was used to control for concurrent effects of demographic variables and predictors on caregiver burden (CBI) and to determine the model’s explanatory power. After verifying the assumptions of linear regression (normality of the dependent variable, independence of errors, and absence of multicollinearity), the independent variables explained 67% of the variance in caregiver burden (R²=0.67, adjusted R²=0.63).
The multiple linear regression results, based on standardized regression coefficients (β) and significance levels (P≤0.05), showed that a history of psychiatric visits (no visits vs visits) was significantly associated with reduced caregiver burden (β=-0.31, P=0.01). Among personality dimensions, extraversion (β=-0.16, P=0.04), openness to experience (β=-0.32, P=0.01), and conscientiousness (β=-0.14, P=0.04) were strongly associated with lower caregiver burden. Additionally, caregivers’ general self-efficacy was significantly linked to reduced caregiver burden (β=-0.10, P=0.04). Other variables such as marital status, employment, and education level were not significantly associated with caregiver burden in the regression model (P>0.05) (Table 4).
Discussion
The present study aimed to determine the association between general self-efficacy and personality traits with caregiver burden among family caregivers of frail elderly in Garmeh County, Iran. More than half of the participants reported high caregiver burden, consistent with prior studies that documented elevated burden prevalence among informal caregivers of older adults, particularly those with frailty, chronic diseases, or disability [37, 38]. This finding underscores the challenges faced by caregivers of frail elderly, who often require prolonged and intensive support, thereby imposing considerable psychological, physical, and social strain on caregivers.
The findings of this study revealed that higher general self-efficacy was significantly associated with lower caregiver burden. Similarly, certain personality traits, namely extraversion, conscientiousness, and openness to experience, exhibited significant inverse associations with caregiver burden and emerged as significant predictors in the multiple regression analysis. The negative association between caregivers’ self-efficacy and caregiver burden (including its dimensions) suggests that higher self-efficacy is likely accompanied by lower burden. This finding is consistent with several prior studies, which emphasize that enhancing caregivers’ perceived competence and confidence can reduce caregiving-related stress, ultimately improving their QoL and functioning [39-41].
Among the personality traits, the dimensions of extraversion, conscientiousness, and openness to experience showed significant negative associations with caregiver burden among family caregivers, a finding consistent with several previous studies [17, 42, 43]. In the present study, extraverted individuals reported lower caregiver burden compared to introverts. The reason may be related to individuals with high extraversion who tend to seek greater social support when facing stress and exhibit more active social behaviors. Additionally, caregivers who score higher on extraversion appear better equipped to manage relational tensions and provide more adaptive responses in stressful situations [17, 44]. Conscientiousness, characterized by traits such as orderliness, responsibility, self-discipline, and diligence (in contrast to disorganization and irresponsibility), suggests that more conscientious and persevering caregivers are likely better able to cope with caregiving stress through structured planning and problem-focused coping strategies. Similarly, caregivers high in openness to experience, characterized by receptiveness to new experiences, curiosity, creativity, and cognitive flexibility, may adopt novel approaches when confronted with new and challenging caregiving situations, thereby achieving better adaptation to caregiving pressures [45]. From a conceptual perspective, self-efficacy and certain personality traits (extraversion, conscientiousness, and openness to experience) may modulate caregiver burden by promoting problem-focused coping, enhancing perceived control, and facilitating the use of social support. However, the cross-sectional design of this study precludes causal inferences regarding these mechanisms.
Univariate analyses revealed significant associations between caregiver burden and occupation, education level, physical illness, and the elderly recipient’s age. However, these associations did not remain significant in the multivariable analysis, aligning with previous studies that reported no significant relationship between caregiver burden and age [46], occupation [39, 47, 48], or physical illness [46, 49]. In contrast, a history of psychiatric visits emerged as a variable that maintained a significant positive association with caregiver burden in the multivariable model. This finding is consistent with the results of studies by Yang et al. [27] and Talebi et al. [50]. Research has shown that the lives of family caregivers are often marked by changes such as time constraints, reduced emotional satisfaction, disruptions in social and family life, self-neglect, and chronic ongoing stress, which can lead to mental health problems. For instance, anxiety and depression negatively affect caregivers’ emotions, thoughts, perceptions, behaviors, and functioning, impairing their ability to optimally perform caregiving tasks and adapt to the situation, thereby increasing caregiver burden [47, 51]. Overall, the findings of this study highlight the prominent and independent role of personal resources, namely self-efficacy and adaptive personality traits, as protective factors, underscoring the need for targeted interventions that emphasize individual differences in this context.
Conclusion
These results cautiously suggest that interventions that enhance caregivers’ self-efficacy, while accounting for individual personality differences, may help alleviate caregiver burden. Accordingly, routine screening for caregiver burden and self-efficacy is recommended at comprehensive health service centers, alongside the implementation of brief educational programs to build coping skills and self-efficacy, and the establishment of clear referral pathways to psychological services for caregivers who exhibit psychiatric symptoms. Furthermore, supportive programs should be tailored to caregivers’ personality profiles, emphasizing self-efficacy enhancement alongside access to psychological counseling and community resources.
Study limitations
The present study has several limitations that should be acknowledged. Its cross-sectional design precludes causal inferences and restricts the examination of temporal changes. All data were gathered through self-report questionnaires at a single time point, potentially introducing social desirability bias. The TIPI scale for personality assessment may be limited by its relatively low internal consistency in older adult populations. Cluster sampling was employed without adjustment for clustering, which may have affected the analyses’ standard errors. Finally, findings were derived from Garmeh County, a region with a unique rural-urban mix in North Khorasan, Iran, limiting generalizability to other cultural, social, or geographic contexts. Future studies should adopt longitudinal designs to establish temporal relationships. Research in more diverse populations would also elucidate the influence of cultural and social factors on caregiver burden.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1403.480). Informed consent was obtained from all participants, and their anonymity was ensured throughout the study. Participants completed a written informed consent form and were informed that they could withdraw from the study at any time without consequences.
Funding
This study was taken from the master’s thesis of Sara Naseripoor, approved by the Department of Geriatric Health, School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, investigation, and data analysis: Ehteram Sadat Ilali and Abdolhakim Jorbonyan; Investigation: Ehteram Sadat Ilali, Abdolhakim Jorbonya, Sara Naseripoor and Abdolhakim Jorbonyan; Data collection, and original draft preparation: Sara Naseripoor and Abdolhakim Jorbonyan; Statistical analysis: Mahmood Moosazadeh; Review and editing: Ehteram Sadat Ilali, Abdolhakim Jorbonyan, and Mahmood Moosazadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Special thanks are extended to all study participants and to the healthcare centers of Garmeh County for their invaluable support and cooperation.
Aging is a natural and inevitable stage of life that is rapidly expanding due to increased life expectancy, declining birth rates, and socio-economic development [1]. This accelerating global aging trend is particularly significant, as it is accompanied by widespread geriatric syndromes that impose substantial healthcare and caregiving burdens on families and health systems [2, 3]. One of the most critical geriatric syndromes is frailty, characterized by decreased physiological resilience to stressors and associated with adverse outcomes, such as disability, functional decline, increased dependency, and reduced quality of life (QoL) [4, 5]. Its prevalence in community-dwelling older adults in Asian countries, based on the fried frailty phenotype, is estimated at 28.0% (95% confidence Interval [CI], 21.3%, 35.3%) [6].
Numerous studies have demonstrated considerable caregiver burden when caring for frail elderly individuals, arising from financial responsibilities, role changes, assistance with activities of daily living, and managing behavioral issues, which can lead to decreased mental health, increased anxiety, maladaptive coping strategies, and reduced quality of care for both caregivers and care recipients [7-9]. This burden can decrease mental health, increase anxiety, maladaptive coping strategies, reduce quality of care, and diminish QoL for both caregiver and care recipient [10, 11]. Despite the availability of formal care services, the primary caregiving role remains with informal family caregivers, who often provide care without formal training and at no cost [12]. Pesantes et al. found that about 95% of the caregiving burden for dependent and disabled individuals falls on family members [13]. This condition exposes family caregivers to diverse physical, emotional, financial, and social challenges [14]. Therefore, identifying factors associated with caregiver burden among family caregivers is crucial.
Research indicates that personal resources and coping abilities play a significant role in reducing caregiver burden [15, 16]. For example, personality traits influence how individuals respond to stress and behave in various situations [17]. Personality is defined as an organized, stable set of relatively enduring characteristics that distinguish individuals [18]. It affects information processing and resistance to opposing views, which are important for caregivers who must make difficult decisions or face conflicting information [19]. Caregivers with higher neuroticism report greater caregiver burden and health problems, while those with higher extraversion scores tend to have better physical and mental health [20, 21]. However, targeting personality traits alone may be limited in effectiveness because they are relatively stable after age 30, highlighting the need to explore other flexible resources that influence caregiver burden [22].
Self-efficacy, as defined by Bandura, refers to an individual’s belief in their capability to execute the actions necessary to manage prospective situations and exert control over events [23]. Higher self-efficacy is associated with greater persistence in the face of challenges, lower perceived stress, and more effective regulation of emotional states; it plays a particularly central role among caregivers, who frequently encounter challenging and unpredictable situations [24]. In this context, studies on family caregivers have demonstrated that greater self-efficacy is linked to improved QoL, enhanced psychological well-being, and better sleep quality among those caring for older adults with chronic illnesses and dementia [25, 26].
Given the strong preference of many older adults for aging in place, the role of family caregivers in contemporary healthcare systems has become increasingly prominent, and the resulting caregiver burden warrants special attention. In this regard, conducting targeted research to identify factors that effectively reduce caregiver burden and enhance care quality is essential, ultimately contributing to the preservation of older adults’ independence and health. A review of the research literature indicates that most studies on caregiver burden have focused on caregivers of individuals with specific diseases, such as dementia or cancer. In contrast, dedicated investigations into family caregivers of frail elderly, characterized by heightened sensitivity to relatively minor stressors, greater dependency, and elevated risks of hospitalization and mortality, remain highly limited, particularly in Iran. Furthermore, examining the roles of psychological factors, such as the big five personality traits and self-efficacy as a positive psychological resource, can provide deeper insights into the determinants of caregiver burden and pave the way for the development of person-centered, evidence-based educational and support interventions. Accordingly, the present study aimed to investigate the associations among self-efficacy, personality traits, and caregiver burden among family caregivers of frail elderly in Garmeh County, North Khorasan Province, Iran.
Materials and Methods
This cross-sectional analytical study was conducted on 243 family caregivers of frail elderly residing in Garmeh County, North Khorasan, Iran, during 2025 (April to June). The study population included all family caregivers of frail elderly living at home and visiting health centers in Garmeh County. The sample size was calculated using G*Power software, version 3.1 with the “exact-correlation: Bivariate normal model” option for a bivariate correlation test, employing an a priori analysis for a two-tailed test based on an effect size (Correlation ρ H1=0.22) from Yang et al. [27], α=0.05, power=0.90, and ρ H0=0, yielding 213 participants corresponding to this specific model. To account for potential non-response, the sample size was increased by 30 participants, bringing the total to 243. Frail elderly were identified from the integrated health care system (SIB) database of Garmeh County based on assessments of nutritional status, body mass index (BMI), mental health status, ability to perform daily activities, need for assistance in personal affairs, dependency status, and need for care.
Sampling was performed by a two-stage random method: First, clusters were selected using cluster sampling from 6 urban comprehensive health service centers and 4 rural health centers. Then, individuals were selected using random sampling (random number table). After obtaining necessary permissions and identifying frail elderly, caregivers (one per frail elderly) were contacted by phone, given verbal consent, and informed about the study objectives. Then, they were invited to participate in health centers. In the next stage, written informed consent was obtained from eligible participants, who were assured of confidentiality. Data collection tools were completed by the caregivers under the researcher’s supervision.
The inclusion criteria included aged 18 years or older, residence in Garmeh County, continuous caregiving for a frail elderly individual for at least the past 6 months, ability to communicate and fluency in Persian, informal caregiver status, no history of psychiatric disorders under treatment (such as schizophrenia, severe depression, cognitive disorders) based on self-report and medical records, and informed consent. The exclusion criterion was incomplete or partially completed questionnaires.
The data collection instruments
Demographic information form included variables such as age, gender, residential status, education level, employment status, income level, physical disease, psychiatric history, history of visits to psychiatrists, and experience of stressful events in the past 6 months.
The general self-efficacy scale (GSE-17) was developed by Sherer et al. in 1982. This scale consists of 17 items [28]. The scoring method is based on a 5-point Likert scale ranging from strongly agree=1 to strongly disagree=5, with a total score range from 17 to 85. Items 1, 3, 8, 9, 13, and 15 are scored directly, while others are reverse-scored. Scores between 17 and 34 indicate low self-efficacy, 34 to 51 moderate self-efficacy, and scores above 51 indicate high self-efficacy [29, 30]. Psychometric properties of the Persian version, including criterion and construct validity, were confirmed by Delavar et al., with a Cronbach α reliability coefficient of 0.79, which is acceptable [31].
The caregiver burden inventory (CBI) assessed caregiver burden using the 24-item version. CBI was developed by Novak and Guest [32]. The inventory consists of 5 subscales: Time-dependent burden (items 1-5), developmental burden (items 6-10), physical burden (items 11-14), social burden (items 15-19), and emotional burden (items 20-24). Responses are rated on a 5-point Likert scale from never (0) to almost always (4). Total scores range from 0 to 96; scores of 36 or higher indicate a high caregiver burden. Internal consistency for the subscales, as measured by Cronbach α in the original inventory, ranged from 0.79 to 0.93 [33]. Shafiezadeh et al. translated and validated the 24-item Persian version, reporting Cronbach α of 0.93 for the total scale and 0.70-0.89 for subscales [34]. In our sample, Cronbach α was 0.94 (total) and 0.89-0.92 (subscales).
The ten-item personality inventory (TIPI) assessed personality traits using Gosling et al.’s 10-item TIPI [35]. The 5 traits measured are extraversion (sociality, sociability), agreeableness (empathy, helpfulness), conscientiousness (orderliness, achievement striving), emotional stability (versus neuroticism), and openness to experience (curiosity, creativity). Each trait is measured with two items. The TIPI is popular due to its cost- and time-efficiency, and can be completed by individuals with minimal literacy. Responses are on a 7-point Likert scale ranging from strongly disagree to agree strongly. Total personality scores range from 10 to 70. Some items are reverse-scored. Gosling et al. [35] reported Cronbach α for subscales between 0.40 and 0.73 in a sample of 1813 participants. In Iran, Azkhosh et al. standardized and localized the scale in a sample of 160 elderly individuals (aged 66 to 71), reporting a Cronbach α of 0.51 for the overall scale and 0.40 to 0.60 for the subscales [36].
Data analysis
The collected data in this study were analyzed using SPSS software, version 26. Initially, the data were screened for outliers. Descriptive statistics, including frequency, percentage, Mean±SD, were used to describe the variables. Inferential statistical tests, including independent t-tests, analysis of variance (ANOVA), Pearson correlation coefficient, and multiple linear regression (simultaneous approach with variables selected based on univariate P<0.2), were employed to examine relationships among variables. The normality of data distribution was assessed using skewness and kurtosis tests. A significance level of less than or equal to 0.05 was considered for all statistical tests.
Results
A total of 243 participants were included in this study. The Mean±SD age of the participants (caregivers) was 51.6±11.3) years. Most participants were married (76.1%), and 90.5% were female. Regarding education, 16.5% of the participants were illiterate. Table 1 presents detailed demographic characteristics of the participants.
Independent t-test results showed that having physical diseases, a history of psychological problems, past psychiatric visits, and experiencing stressful events in the last 6 months were significantly associated with increased caregiver burden (P≤0.05). However, no significant association was found between caregiver burden and the gender of the caregiver or the older person, or residential status (P> 0.05) (Table 1).
ANOVA revealed significant differences in mean caregiver burden scores across groups classified by caregivers’ education level, employment status, and the age group of the cared-for elderly (P≤0.05) (Table 1). Post-hoc Tukey tests revealed that caregivers of older people aged 60-74 years experienced significantly lower burden than those caring for those aged ≥85 years (P<0.01). University-educated caregivers reported lower burden than those with primary education (P<0.01). Homemakers had a higher burden than employed (P<0.01) and retired caregivers (P<0.05). No significant differences were found for caregiving duration, living arrangement, or relationship to older people (P>0.05) (Table 1).
Normality test results based on skewness and kurtosis indicated that the data were within the acceptable range (-2 to +2), confirming normality. The Mean±SD score of the CBI was 42.32(18.81). Of 247 caregivers, 126(51%) had CBI scores ≥36, confirming substantial prevalence of high caregiver burden. Among the caregiver burden components, emotional burden had the highest Mean±SD score of 11.17(5.06). Descriptive statistics of the quantitative variables are presented in Table 2.
The correlation analysis results revealed a significant negative association between general self-efficacy and CBI in the present study (r=-0.56, P≤0.05). This finding indicates that as caregivers’ self-efficacy levels increase, their caregiver burden decreases. Among the caregiver burden subscales, emotional burden showed the strongest negative correlation with self-efficacy (r=-0.57, P≤0.001), whereas physical burden had the weakest correlation (r=-0.40, P<0.001) (Table 3).
Additionally, caregiver burden was significantly and negatively correlated with personality traits (P≤0.05). Among these, extraversion (r=-0.67, P<0.05) and openness to experience (r=-0.70, P<0.05) had the strongest associations with caregiver burden. This finding suggests that individuals who are more extraverted and open to new experiences experience less caregiver burden. No significant association was found between caregiver age and overall CBI (P≥0.05); however, positive and significant correlations were observed between age and physical burden (r=0.28, P≤0.05) as well as time-dependent burden (r=0.26, P≤0.05) (Table 3).
In this study, a simultaneous multiple regression analysis was used to control for concurrent effects of demographic variables and predictors on caregiver burden (CBI) and to determine the model’s explanatory power. After verifying the assumptions of linear regression (normality of the dependent variable, independence of errors, and absence of multicollinearity), the independent variables explained 67% of the variance in caregiver burden (R²=0.67, adjusted R²=0.63).
The multiple linear regression results, based on standardized regression coefficients (β) and significance levels (P≤0.05), showed that a history of psychiatric visits (no visits vs visits) was significantly associated with reduced caregiver burden (β=-0.31, P=0.01). Among personality dimensions, extraversion (β=-0.16, P=0.04), openness to experience (β=-0.32, P=0.01), and conscientiousness (β=-0.14, P=0.04) were strongly associated with lower caregiver burden. Additionally, caregivers’ general self-efficacy was significantly linked to reduced caregiver burden (β=-0.10, P=0.04). Other variables such as marital status, employment, and education level were not significantly associated with caregiver burden in the regression model (P>0.05) (Table 4).
Discussion
The present study aimed to determine the association between general self-efficacy and personality traits with caregiver burden among family caregivers of frail elderly in Garmeh County, Iran. More than half of the participants reported high caregiver burden, consistent with prior studies that documented elevated burden prevalence among informal caregivers of older adults, particularly those with frailty, chronic diseases, or disability [37, 38]. This finding underscores the challenges faced by caregivers of frail elderly, who often require prolonged and intensive support, thereby imposing considerable psychological, physical, and social strain on caregivers.
The findings of this study revealed that higher general self-efficacy was significantly associated with lower caregiver burden. Similarly, certain personality traits, namely extraversion, conscientiousness, and openness to experience, exhibited significant inverse associations with caregiver burden and emerged as significant predictors in the multiple regression analysis. The negative association between caregivers’ self-efficacy and caregiver burden (including its dimensions) suggests that higher self-efficacy is likely accompanied by lower burden. This finding is consistent with several prior studies, which emphasize that enhancing caregivers’ perceived competence and confidence can reduce caregiving-related stress, ultimately improving their QoL and functioning [39-41].
Among the personality traits, the dimensions of extraversion, conscientiousness, and openness to experience showed significant negative associations with caregiver burden among family caregivers, a finding consistent with several previous studies [17, 42, 43]. In the present study, extraverted individuals reported lower caregiver burden compared to introverts. The reason may be related to individuals with high extraversion who tend to seek greater social support when facing stress and exhibit more active social behaviors. Additionally, caregivers who score higher on extraversion appear better equipped to manage relational tensions and provide more adaptive responses in stressful situations [17, 44]. Conscientiousness, characterized by traits such as orderliness, responsibility, self-discipline, and diligence (in contrast to disorganization and irresponsibility), suggests that more conscientious and persevering caregivers are likely better able to cope with caregiving stress through structured planning and problem-focused coping strategies. Similarly, caregivers high in openness to experience, characterized by receptiveness to new experiences, curiosity, creativity, and cognitive flexibility, may adopt novel approaches when confronted with new and challenging caregiving situations, thereby achieving better adaptation to caregiving pressures [45]. From a conceptual perspective, self-efficacy and certain personality traits (extraversion, conscientiousness, and openness to experience) may modulate caregiver burden by promoting problem-focused coping, enhancing perceived control, and facilitating the use of social support. However, the cross-sectional design of this study precludes causal inferences regarding these mechanisms.
Univariate analyses revealed significant associations between caregiver burden and occupation, education level, physical illness, and the elderly recipient’s age. However, these associations did not remain significant in the multivariable analysis, aligning with previous studies that reported no significant relationship between caregiver burden and age [46], occupation [39, 47, 48], or physical illness [46, 49]. In contrast, a history of psychiatric visits emerged as a variable that maintained a significant positive association with caregiver burden in the multivariable model. This finding is consistent with the results of studies by Yang et al. [27] and Talebi et al. [50]. Research has shown that the lives of family caregivers are often marked by changes such as time constraints, reduced emotional satisfaction, disruptions in social and family life, self-neglect, and chronic ongoing stress, which can lead to mental health problems. For instance, anxiety and depression negatively affect caregivers’ emotions, thoughts, perceptions, behaviors, and functioning, impairing their ability to optimally perform caregiving tasks and adapt to the situation, thereby increasing caregiver burden [47, 51]. Overall, the findings of this study highlight the prominent and independent role of personal resources, namely self-efficacy and adaptive personality traits, as protective factors, underscoring the need for targeted interventions that emphasize individual differences in this context.
Conclusion
These results cautiously suggest that interventions that enhance caregivers’ self-efficacy, while accounting for individual personality differences, may help alleviate caregiver burden. Accordingly, routine screening for caregiver burden and self-efficacy is recommended at comprehensive health service centers, alongside the implementation of brief educational programs to build coping skills and self-efficacy, and the establishment of clear referral pathways to psychological services for caregivers who exhibit psychiatric symptoms. Furthermore, supportive programs should be tailored to caregivers’ personality profiles, emphasizing self-efficacy enhancement alongside access to psychological counseling and community resources.
Study limitations
The present study has several limitations that should be acknowledged. Its cross-sectional design precludes causal inferences and restricts the examination of temporal changes. All data were gathered through self-report questionnaires at a single time point, potentially introducing social desirability bias. The TIPI scale for personality assessment may be limited by its relatively low internal consistency in older adult populations. Cluster sampling was employed without adjustment for clustering, which may have affected the analyses’ standard errors. Finally, findings were derived from Garmeh County, a region with a unique rural-urban mix in North Khorasan, Iran, limiting generalizability to other cultural, social, or geographic contexts. Future studies should adopt longitudinal designs to establish temporal relationships. Research in more diverse populations would also elucidate the influence of cultural and social factors on caregiver burden.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1403.480). Informed consent was obtained from all participants, and their anonymity was ensured throughout the study. Participants completed a written informed consent form and were informed that they could withdraw from the study at any time without consequences.
Funding
This study was taken from the master’s thesis of Sara Naseripoor, approved by the Department of Geriatric Health, School of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran. This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, study design, investigation, and data analysis: Ehteram Sadat Ilali and Abdolhakim Jorbonyan; Investigation: Ehteram Sadat Ilali, Abdolhakim Jorbonya, Sara Naseripoor and Abdolhakim Jorbonyan; Data collection, and original draft preparation: Sara Naseripoor and Abdolhakim Jorbonyan; Statistical analysis: Mahmood Moosazadeh; Review and editing: Ehteram Sadat Ilali, Abdolhakim Jorbonyan, and Mahmood Moosazadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Special thanks are extended to all study participants and to the healthcare centers of Garmeh County for their invaluable support and cooperation.
References
- Abbasi-Shavazi M, Jambarsang S, Anbari-Nogyni Z, Sadeghian H, Anoosheh VS. Examining fall risk and related factors in rural older adults: A cross-sectional study in Yazd Province, Iran. Iranian Journal of Health Sciences. 2024;12(2):99-108. [DOI:10.32598/ijhs.12.2.1013.1]
- Jafari M, Alipour F, Raheb G, Mardani M. [Perceived stress and burden of care in elderly caregivers: The moderating role of resilience (Persian)]. Salmand: Iranian Journal of Ageing. 2022; 17(1):62-75. [DOI:10.32598/sija.2021.2575.2]
- Sanford AM, Morley JE, Berg-Weger M, Lundy J, Little MO, Leonard K, et al. High prevalence of geriatric syndromes in older adults. PLoS One. 2020;15(6):e0233857. [DOI:10.1371/journal.pone.0233857] [PMID]
- Blodgett JM, Theou O, Howlett SE, Wu FC, Rockwood K. A frailty index based on laboratory deficits in community-dwelling men predicted their risk of adverse health outcomes. Age and Ageing. 2016; 45(4):463-8. [DOI:10.1093/ageing/afw054] [PMID]
- Nikaeen R, Khalilian A, Bahrampour A. Determining the effective factors on gastric cancer using frailty model in South-East and North of Iran. Iranian Journal of Health Sciences. 2017; 5(3):35-48. [DOI:10.29252/jhs.5.3.35]
- To TL, Doan TN, Ho WC, Liao WC. Prevalence of frailty among community-dwelling older adults in Asian countries: A systematic review and meta-analysis. Healthcare (Basel). 2022; 10(5):895. [DOI:10.3390/healthcare10050895] [PMID]
- Chindaprasirt J, Limpawattana P, Pakkaratho P, Wirasorn K, Sookprasert A, Kongbunkiat K, et al. Burdens among caregivers of older adults with advanced cancer and risk factors. Asian Pacific Journal of Cancer Prevention. 2014; 15(4):1643-8. [DOI:10.7314/APJCP.2014.15.4.1643] [PMID]
- Sezgin H, Cevheroglu S, Gök ND. Effects of care burden on the life of caregivers of the elderly: A mixed-method study model. Medicine (Baltimore). 2022; 101(43):e30736. [DOI:10.1097/MD.0000000000030736] [PMID]
- Chan CY, De Roza JG, Ding GTY, Koh HL, Lee ES. Psychosocial factors and caregiver burden among primary family caregivers of frail older adults with multimorbidity. BMC Primary Care. 2023; 24(1):36. [DOI:10.1186/s12875-023-01985-y] [PMID]
- Tziaka E, Tsiakiri A, Vlotinou P, Christidi F, Tsiptsios D, Aggelousis N, et al. A holistic approach to expressing the burden of caregivers for stroke survivors: A systematic review. Healthcare (Basel). 2024; 12(5):565. [DOI:10.3390/healthcare12050565] [PMID]
- Dadashi-Tonkaboni N, Peyman N. Social support on family caregivers of Alzheimer patients: A systematic review. Iranian Journal of Health Sciences. 2023; 11(3):157-64. [DOI:10.32598/ijhs.11.3.933.1]
- Marinho JS, Batista IB, Nobre RAS, Guimarães MSA, Santos-Orlandi AAS, Brito TRP, et al. Burden, satisfaction caregiving, and family relations in informal caregivers of older adults. Frontiers in Medicine. 2022; 9:1059467. [DOI:10.3389/fmed.2022.1059467] [PMID]
- Pesantes MA, Brandt LR, Ipince A, Miranda JJ, Diez-Canseco F. An exploration into caring for a stroke survivor in Lima, Peru: Emotional impact, stress factors, coping mechanisms and unmet needs of informal caregivers. ENeurologicalSci. 2017; 6:33-50. [DOI:10.1016/j.ensci.2016.11.004] [PMID]
- Alizadeh M, Hoseini M, Shojaeizadeh D, Rahimi A, Arshinchi M, Rohani H. [Assessing anxiety, depression and psychological wellbeing status of urban elderly in Tehran metropolitan city (Persian)]. Iranian Journal of Ageing. 2012; 7(3):66-73. [Link]
- Long D, Gu Y, Wang Y. Sense of coherence and caregiver burden among informal caregivers of people with dementia in China: The mediating role of coping strategies. Psychology Research and Behavior Management. 2025; 18:1423-33. [DOI:10.2147/PRBM.S518799] [PMID]
- Lv R, Yang L, Li J, Kuang J, Zhou K, Xu M. Depression mediates the association between burden and quality of life in informal caregivers of stroke survivors: Meta-analytic structural equation modeling. Archives of Physical Medicine and Rehabilitation. 2024; 105(10):1961-70. [DOI:10.1016/j.apmr.2024.01.022] [PMID]
- Kim SK, Park M, Lee Y, Choi SH, Moon SY, Seo SW, et al. Influence of personality on depression, burden, and health-related quality of life in family caregivers of persons with dementia. International Psychogeriatrics. 2017; 29(2):227-37. [DOI:10.1017/S1041610216001770] [PMID]
- Yunus M, Wahab NBA, Ismail MS, Othman MS. The important role of personality trait. International Journal of Academic Research in Business and Social Sciences. 2018; 8(7):1028-36. [DOI:10.6007/IJARBSS/v8-i7/4530]
- Valli C, Nai A. Dispositioned to resist? The Big Five and resistance to dissonant political views. Personality and Individual Differences. 2023; 207:112152. [DOI:10.1016/j.paid.2023.112152]
- Abbasi M, Mirderikvand F, Adavi H, Hojati M. [The relationship between personality traits (neuroticism and extraversion) and self-efficacy with aging depression (Persian)]. Salmand: Iranian Journal of Ageing. 2018; 12(4):458-66. [DOI:10.21859/sija.12.4.458]
- Hajek A, König HH. The relation between personality, informal caregiving, life satisfaction and health-related quality of life: Evidence of a longitudinal study. Quality of Life Research. 2018; 27(5):1249-56. [DOI:10.1007/s11136-018-1787-6] [PMID]
- Löckenhoff CE, Duberstein PR, Friedman B, Costa PT Jr. Five-factor personality traits and subjective health among caregivers: The role of caregiver strain and self-efficacy. Psychology and Aging. 2011; 26(3):592-604. [DOI:10.1037/a0022209] [PMID]
- Bandura A. Guide for constructing self-efficacy scales. In: Pajares F, Urdan T, editors. Self-efficacy beliefs of adolescents. 2006. [DOI:10.1108/978-1-60752-750-3]
- Singh B, Udainiya R. Self-efficacy and wellbeing of adolescents. Journal of the Indian Academy of Applied psychology. 2009; 35(2):227-32. [Link]
- Yagil D, Medler-Liraz H, Bichachi R. Mindfulness and self-efficacy enhance employee performance by reducing stress. Personality and Individual Differences. 2023; 207:112150. [DOI:10.1016/j.paid.2023.112150]
- Uslu A, Polat Ü. Self-efficacy, quality of life and care burden in caregivers of patients with dementia. Journal of General Health Sciences. 2022; 4(2):106-17. [DOI:10.51123/jgehes.2022.48]
- Yang Z, Sun F, Zhao L, Hu T, Lin X, Guo Y. Self-efficacy and wellbeing in the association between caregiver burden and sleep quality among caregivers of elderly patients with multiple chronic conditions in rural China: A serial multiple mediation analysis. BMC Nursing. 2023; 22(1):424. [DOI:10.1186/s12912-023-01587-0] [PMID]
- Sherer M, Adams CH. Construct validation of the self-efficacy scale. Psychological Reports. 1983; 53(3):899-902. [DOI:10.2466/pr0.1983.53.3.899]
- Haghayegh A, Ghasemi N, Neshardoost HT, Kajbaf MB, Khanbani M. [Psychometric properties of diabetes management (Persian)]. Iranian Journal of Endocrinology and Metabolism. 2010; 12 (2):111-5. [Link]
- Sefidi F, Farzad V. Validated measure of Ryff psychological wellbeing among students of Qazvin University of Medical Sciences (2009). Journal of Inflammatory Diseases. 2012; 16(1):65-71. [Link]
- Delavar A, Najafi M. [The psychometric properties of the general self-efficacy scale among university staff (Persian)]. Quarterly of Educational Measurement. 2013; 4(12):87-104. [Link]
- Novak M, Guest C. A comparison of the impact of institutionalization on spouse and nonspouse caregivers. Journal of Applied Gerontology. 1992; 11(4):379-94. [DOI:10.1177/073346489201100401] [PMID]
- Chou KR, Jiann-Chyun L, Chu H. The reliability and validity of the Chinese version of the caregiver burden inventory. Nursing Research. 2002; 51(5):324-31. [DOI:10.1097/00006199-200209000-00009] [PMID]
- Shafiezadeh A, Heravi-Karimoo M, Rejeh N, Sharif Nia H, Montazeri A. [Translation and primary validation of the Persian version of caregiver burden inventory (Persian)]. Payesh. 2019; 18(4):405-14. [Link]
- Gosling SD, Rentfrow PJ, Swann WB Jr. A very brief measure of the Big-Five personality domains. Journal of Research in Personality. 2003; 37(6):504-28. [DOI:10.1016/S0092-6566(03)00046-1]
- Manoochehr A, Robab S, Mohammad R, Amir A. Reliability and validity of the 10-item personality inventory among older Iranians. Psychology in Russia: State of the Art. 2019; 12(3):29-40. [DOI:10.11621/pir.2019.0303]
- Ding TYG, De Roza JG, Chan CY, Lee PSS, Ong SK, Lew KJ, et al. Factors associated with family caregiver burden among frail older persons with multimorbidity. BMC Geriatrics. 2022; 22(1):160. [DOI:10.1186/s12877-022-02858-2] [PMID]
- Madani SF, Farokhzad P. [Investigating the effectiveness of compassion-focused therapy on caregiver burden and psychological flexibility in caregivers of elderly with Alzheimer disease (Persian)]. Salmand: Iranian Journal of Ageing. 2025; 20(1):122-35. [DOI:10.32598/sija.2024.3786.1]
- Shankar KN, Hirschman KB, Hanlon AL, Naylor MD. Burden in caregivers of cognitively impaired elderly adults at time of hospitalization: A cross-sectional analysis. Journal of the American Geriatrics Society. 2014; 62(2):276-84. [DOI:10.1111/jgs.12657] [PMID]
- Banitalebi S, Etemadifar S, Kheiri S, Masoudi R. The effect of a self-management program on care burden and self-efficacy in family caregivers of people with multiple sclerosis. The Journal of Nursing Research. 2022; 30(5):e234. [DOI:10.1097/jnr.0000000000000509] [PMID]
- Grano C, Lucidi F, Violani C. The relationship between caregiving self-efficacy and depressive symptoms in family caregivers of patients with Alzheimer disease: A longitudinal study. International Psychogeriatrics. 2017; 29(7):1095-103. [DOI:10.1017/S1041610217000059] [PMID]
- Luchetti M, Terracciano A, Stephan Y, Aschwanden D, Sutin AR. Personality and psychological health in caregivers of older relatives: A case-control study. Aging & Mental Health. 2021; 25(9):1692-700. [DOI:10.1080/13607863.2020.1758907] [PMID]
- Rahimzadehsani M, Momtaz YA, Foroughan M, Zanjari N. [The relationship between personality traits of older adults and elder abuse (Persian)]. Salmand: Iranian Journal of Ageing. 2023; 18(1):92-103. [DOI:10.32598/sija.2022.3436.1]
- Melo G, Maroco J, De Mendonça AJ. Influence of personality on caregiver burden, depression and distress related to BPSD. International Journal of Geriatric Psychiatry. 2011; 26(12):1275-82. [DOI:10.1002/gps.2677] [PMID]
- Ju P, Lohmar S, Fenstermacher E, Owsiany M, Edelstein B. Personality traits as predictors of burnout in sandwich generation caregivers. Innovation in Aging. 2024; 8(Suppl 1):770. [DOI:10.1093/geroni/igae098.2502]
- Noguchi T, Nakagawa-Senda H, Tamai Y, Nishiyama T, Watanabe M, Kamiya M, et al., editors. The association between family caregiver burden and subjective wellbeing and the moderating effect of social participation among Japanese adults: A cross-sectional study. Healthcare (Basel). 2020; 8(2):87. [DOI:10.3390/healthcare8020087] [PMID]
- Avazzadeh S, Gilani N, Jahangiry L. Predictors of fear control related to COVID-19 among older population: COVID-19 risk perception and health-related quality of life during the pandemic. Health and quality of Life Outcomes. 2023; 21(1):79. [DOI:10.1186/s12955-023-02167-1] [PMID]
- Scott CB. Alzheimer’s disease caregiver burden: Does resilience matter? Journal of Human Behavior in the Social Environment. 2013; 23(8):879-92. [DOI:10.1080/10911359.2013.803451]
- Senturk SG, Akyol MA, Kucukguclu O. The relationship between caregiver burden and psychological resilience in caregivers of individuals with dementia. International Journal of Caring Sciences. 2018; 11(2):1223-30. [Link]
- Talebi M, Mokhtari LN, Rezasoltani P, Kazemnejad LE, Shamsizadeh M. [Caregiver burden in caregivers of renal patients under hemodialysis (Persian)]. Journal Of Holistic Nursing And Midwifery. 2016; 25(80):59-86. [Link]
- Kim EK, Park H. Factors associated with burden of family caregivers of home-dwelling elderly people with dementia: A systematic review and meta-analysis. Korean J Adult Nurs. 2019; 31(4):351-64. [DOI:10.7475/kjan.2019.31.4.351]
Type of Study: Original Article |
Subject:
Geriatrics
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
