

Volume 12, Issue 2 (Spring 2024)
Iran J Health Sci 2024, 12(2): 99-108 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abbasi-Shavazi M, Jambarsang S, Anbari-Nogyni Z, Sadeghian H, Anoosheh V S. Examining Fall Risk and Related Factors in Rural Older Adults: A Cross-sectional Study in Yazd Province, Iran. Iran J Health Sci 2024; 12 (2) :99-108
URL: http://jhs.mazums.ac.ir/article-1-922-en.html
URL: http://jhs.mazums.ac.ir/article-1-922-en.html
Masoumeh Abbasi-Shavazi 

 , Sara Jambarsang , Zainab Anbari-Nogyni * , Hosseinali Sadeghian , Vida Sadat Anoosheh
, Sara Jambarsang , Zainab Anbari-Nogyni * , Hosseinali Sadeghian , Vida Sadat Anoosheh
, Sara Jambarsang , Zainab Anbari-Nogyni * , Hosseinali Sadeghian , Vida Sadat Anoosheh
Elderly Health Research Center, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. , zai.anbari@uswr.ac.ir
Full-Text [PDF 768 kb]
(1047 Downloads)
| Abstract (HTML) (3709 Views)
Full-Text: (1721 Views)
Introduction
According to the forecasts of the current statistics, the world’s elderly population in 2030 will grow from 9% to 16% and in Iran from 6.5% to 17.5% [1]. Evidence suggests that increasing age is strongly associated with functional disorders [2], decreased muscle strength, neural function, physiological function [3] and decreased balance [4]. Also, elderly people are exposed to various diseases because of physiological and pathological changes [5]. Balance and gait disorders are the most common causes of falls in the elderly [6] and the changes in gait in the elderly are often related to underlying conditions, such as illness, especially, increased severity of illness [7]. The prevalence of falls among the elderly was also reported at 27.6%, 30.0%, and 46.8% in other studies [8, 9, 10].
Maintaining balance is a physiological process [3], an essential skill in avoiding falls [7] and an indispensable factor for active participation and contribution to the community [11]. Falls in the elderly population are a major public health problem because they lead to premature mortality and individuals who survive sustain significant losses to their quality of life [12]. Falls can limit daily activities and cause syndromes, such as dependence, immobility and depressive disorder [13]. The results of some studies showed that the increase in age and associated diseases decrease the average score of physical activity in the elderly population [14].
In addition to physical injuries, recurrent falls can have a significant psychological impact. Fear of falling again (post-fall syndrome) can lead elderly individuals to become so afraid of moving that they restrict their activity levels [15]. Some studies have reported risk factors related to imbalance, including diabetes, arthritis, mental disorder [16], falling and reflex, pain, power loss [17], delirium, dementia, Parkinson disease, vitamin B12 deficiency, obesity and stroke [6]. Some other studies in Iran considered factors, such as gender, daily living activity, physical activity, number of diseases and quadriceps muscle strength as the causes of imbalances [20].
The fall accounts for one of the most important factors affecting the onset of functional disorders [21], causing many problems, including increased possibility of falls, reduced independence [11], increased health care needs and level of mortality rates and reduced quality of life related to movement limitation in older people [20]. According to the Iranian elderly health survey in 2015-2016, about 40% of the elderly have gait disorders and 33% use assistive devices. This study also showed that 60% of the elderly were completely dependent on daily activities and 54% had balance disorders [16]. The rural elderly are more at risk compared to urban elderly people due to various aspects, such as education, economic status and health care access. These aspects highlight the importance of studying the balanced status of the rural elderly [19].
Considering the increasing number of elderly and the high prevalence of movement disorders, the risk of falls, and disability in this age group, it is necessary to study the balance in the elderly. On the other hand, the information related to the epidemiology of falls and related factors in rural elderly is limited; therefore, fall risk assessment of the elderly and identifying the major risk factors in this population can provide the appropriate context for practical planning to prevent falls and subsequent disabilities. Accordingly, this study evaluates the balance status and identifies risk factors in the rural elderly of Yazd Province, Iran.
Materials and Methods
Study participants
This cross-sectional study was conducted in rural areas of Yazd Province, Iran, using multi-stage sampling. The participants included 302 elderly people aged over 60 years, considering d=0.6 and s=5.06 (obtained from the pilot study), a power of 80% and an attrition rate of 10%. Firstly, four cities out of 12 cities in Yazd Province, Iran, were randomly selected and one rural healthcare center was selected for sampling in each city. Since the elderly in Iran are provided with inclusive healthcare services and are under healthcare coverage, after listing the names of the elderly covered in the selected rural health centers in each city, approximately 75 people were selected from each center using the systematic random sampling method and invited to participate in the study. The inclusion criteria were the ability to communicate, not taking more than two drugs at the same time in the past 24 h, no dizziness and headache during testing, no psychotropic medication, appropriate diastolic and systolic blood pressure, a lack of severe cognitive disabilities or dementia and the ability to understand verbal instructions. The criteria were identified based on the clinical records of the elderly and their reports.
Data collection instruments
In this study, a multi-section questionnaire, including demographic questions (age, gender, education, tobacco use, history of illness and falls) as well as a questionnaire for assessing gait and balance in the elderly named Tinetti performance oriented mobility assessment (POMA) was used. POMA is an easy adjunctive test that measures gait and balance in the elderly during daily activities. Tinetti gait and balance scale is a reliable and clinically valid tool [21] And It may be a more useful measure than BBS or TUG in patients with impaired dynamic balance or reactive balance during walking [22]. It is one of the best options for assessing the risk of mobility disorders in the elderly [23]. It takes 10 to 15 min and provides the patients with the ability to perform a specific task. Initial scoring tools are performed on three sequential ratings of 0 to 2. A score of 0 indicates a high defect, while a score of 2 indicates the patient’s independence. Each score is a combination of three measures, including gait, balance assessment score and total score. The maximum score is 12 for gait, the maximum for balance is 16, and the total score is 28. Overall, a score below 19 is regarded as a high risk of falls, a score between 19 and 23 identifies a moderate risk, and a score of 24 or higher indicates a low fall risk [24, 25]. The psychometric characteristics of this tool were evaluated and approved in the previous study by Mazloomy Mahmoodabad et al. conducted on Iranian elderly [26]. The questionnaire was completed by trained interviewers who were among the healthcare providers. The subjects were invited to the healthcare center and the questionnaire and checklist were completed for them in a safe place of the healthcare center.
Statistical analysis
Statistical analysis was performed using the SPSS software, version 20. Frequency distribution, Mean±SD were calculated after the normality test using the Kolmogorov-Smirnov test. A chi-square test was used to compare the qualitative variables. Also, the relationship between significant variables with the risk of falls was measured using the ordinal logistic regression model based on the chi-square test. The statistical significance level of P<0.05 was considered in all tests.
Results
This study included 302 elderly people with a mean age of 75.08±6.72 years, most of whom (54%) were aged between 70 and 80 years. Also, 189(62.6%) of the participants were illiterate and 162(54.6%) were female. The percentages of hypertension, arthritis, vision disorders and diabetes were 175(57.9%), 170(56.3%), 99(32.8%) and 87(28.8%), respectively (Table 1).
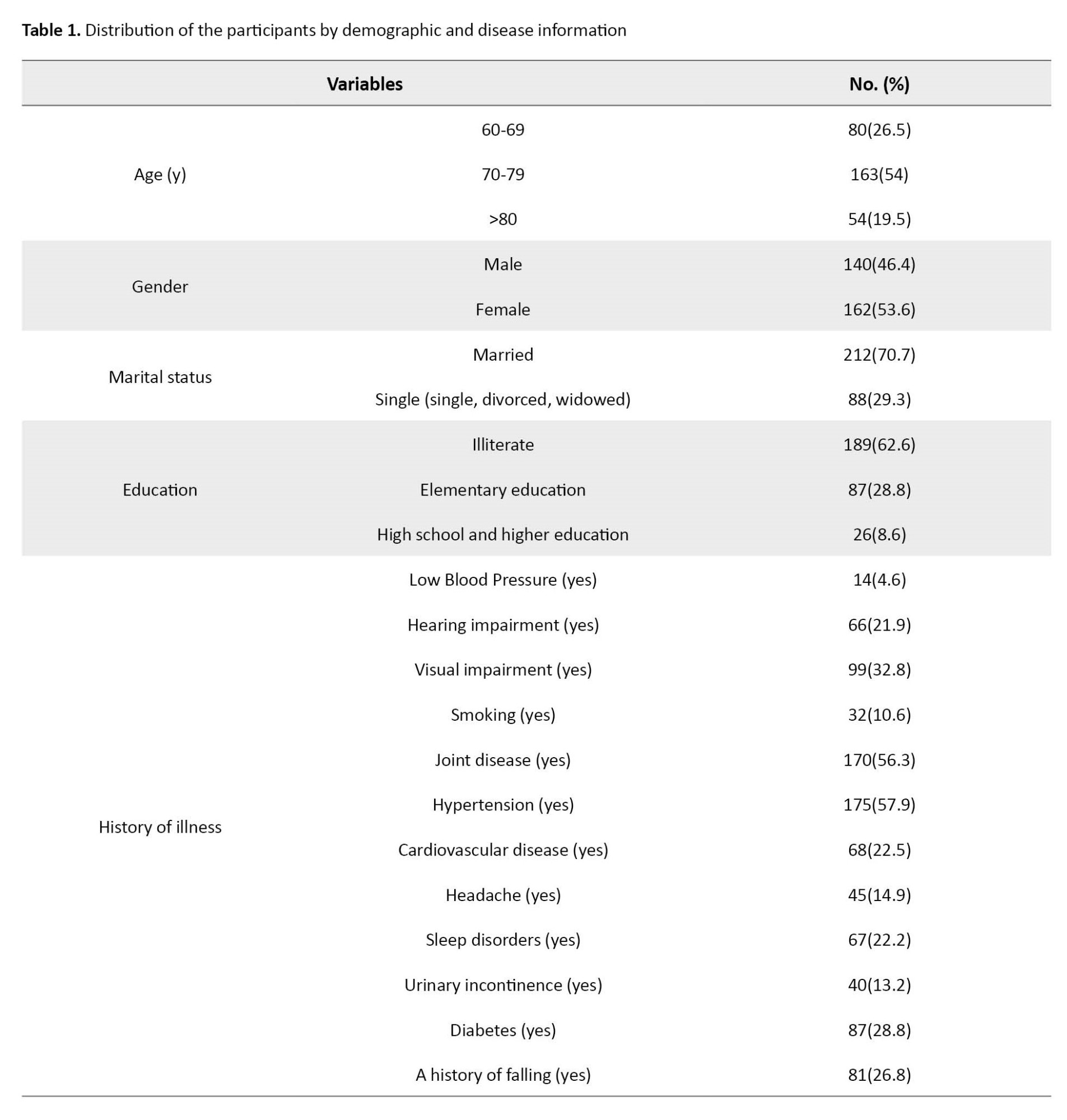
Table 2 shows the distribution of the participants risk of falls by demographic and disease information.
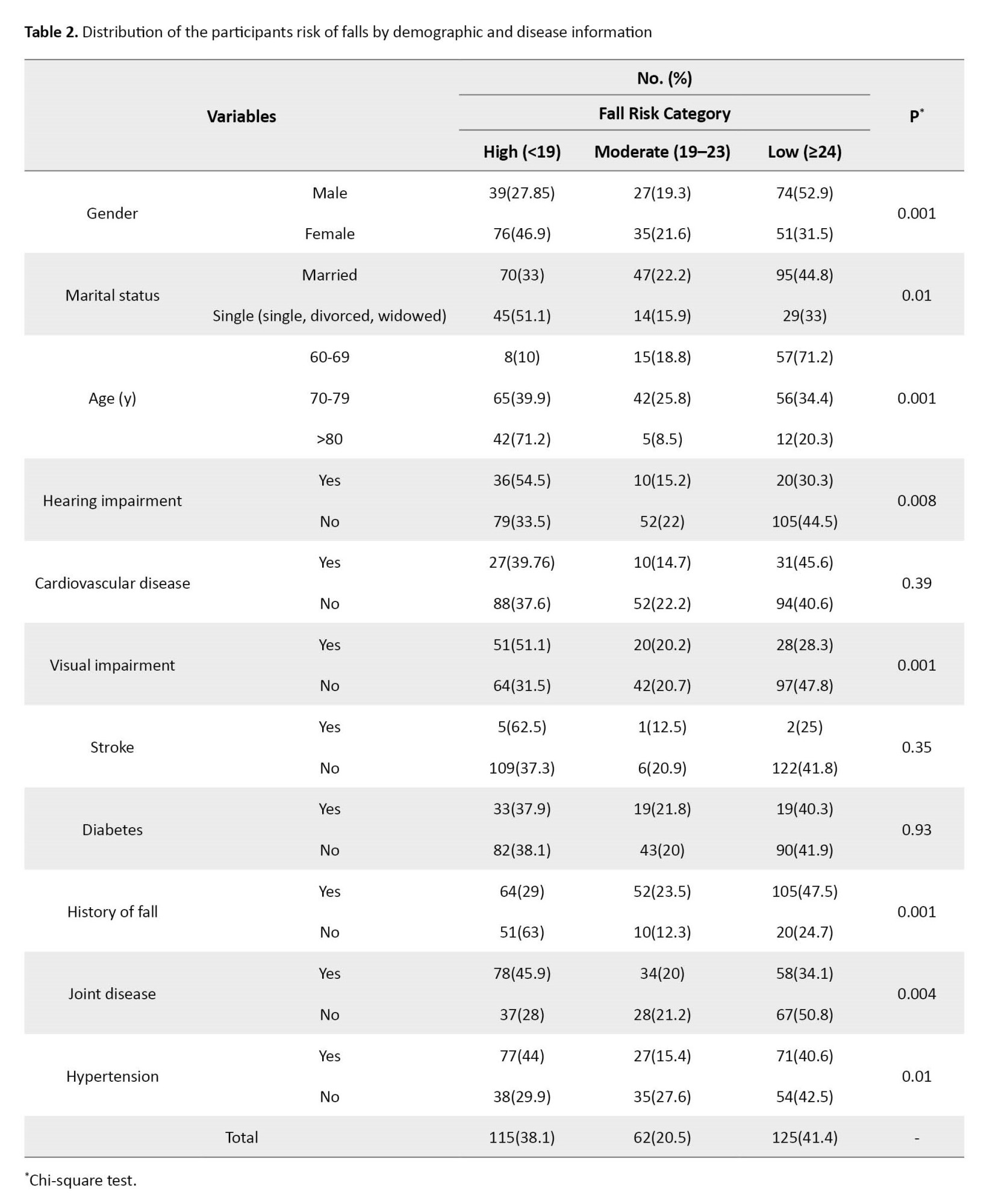
In terms of risk of falls, 115(38.1%) of the participants were in the high-risk group, 62(20.5%) in the medium-risk group, and 125(41.4%) in the low-risk group. According to the results of the X2 test, the risk of falls was significantly related to gender. Most female subjects (46.9%) were at high fall risk and most male subjects (52.9%) were at low fall risk. Also, 54.5% and 51.5% of the subjects with hearing and visual impairment were at high fall risk, respectively. On the other hand, 45.9% of arthritis patients and 44% of hypertensive patients were at high fall risk. In addition, 51.5% and 71.2% of the elderly, lonely, and elderly aged over 80 years were at high fall risk, respectively (P<0.05).
The odds ratio (OR) with a 95% confidence interval (CI) for investigating the association of the risk of falls with some variables is shown in Table 3.
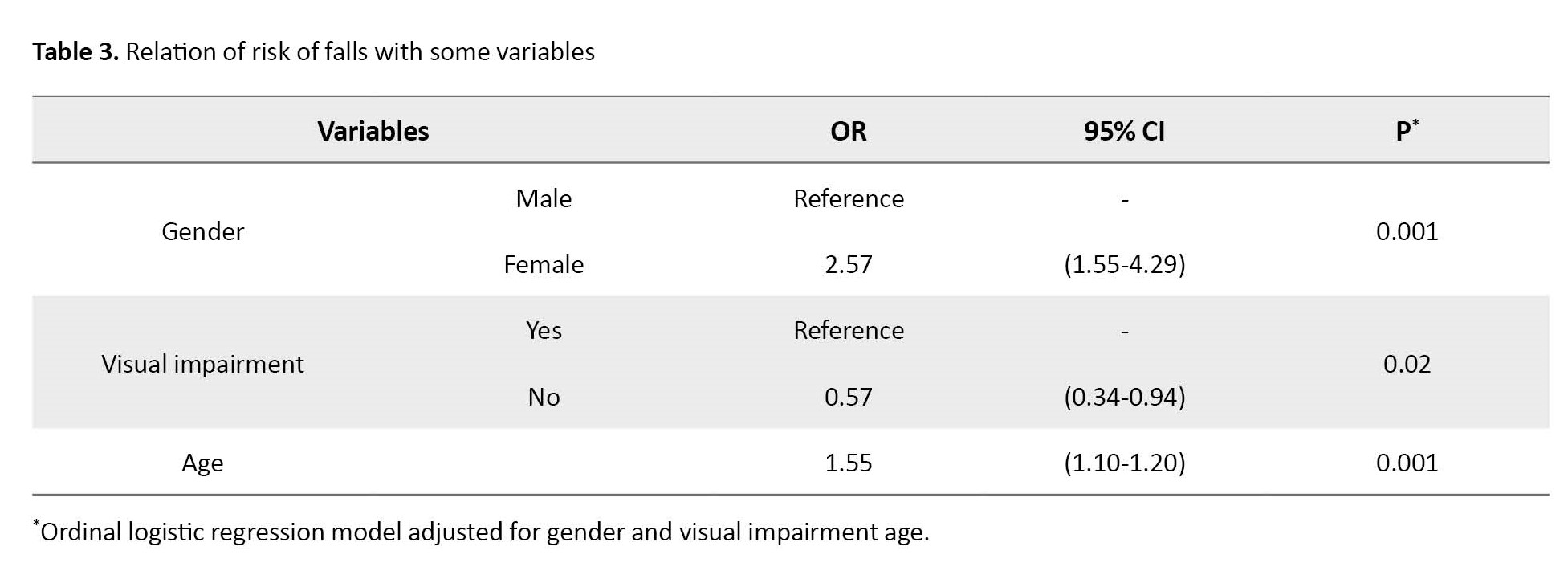
According to the chi-square table, the variables with P<0.3 were included in the ordinal logistic regression model. Based on the ordinal logistic model, the relationship between significant variables with moderating effects of other variables (gender, marital status, visual and auditory impairments, history of falls, hypertension and arthritis) on the risk of falls was investigated. The results showed that gender, age and visual status had a significant effect on the risk of falls in the elderly (P<0.05). The probability of falls in women was 2.6 times higher than in men. Also, the probability of falls in people with visual impairment was 1.7 times higher than those with no visual impairment. In addition, the probability of falls was 15% higher in the elderly as they get older.
Discussion
This study investigated the balance and factors affecting the risk of falls in the elderly population in Yazd Province, Iran. The results showed that 38.1% of the subjects presented a high fall risk, 20.5% were medium risk and 41.4% showed a low fall risk. The study in Riyadh, Saudi Arabia, showed that 44.5% of people were at high risk of falls, 32.8% were at moderate to severe risk of falls and 22.7% were not at risk of falls [27], which is not in line with the present study. On the other hand, the study by Zarepour in Urmia City, Iran, reported that 47.1%, 42.9% and 10% of the elderly had a severe, moderate and low risk of falls, respectively [28]. A study on the elderly, using the Berg instrument showed that 7.5% of the participants were at moderate or severe and 92.5% were at low risk of fall [29]. The observed differences in the results of surveys on the risk of falls can be explained by differences in the characteristics of participants (urban or rural, different age groups, health conditions), measurement tools for risk assessment of falls, and sample size of participants.
The results showed a significant relationship between visual impairment and the risk of falls in the elderly, which is consistent with previous studies [25, 30, 31]. In the cross-sectional study by Aartolahti et al. on the elderly aged over 76 years, people with poor visual function had significantly lower balance and mobility compared to those with moderate or good visual function [25]. Similarly, the study by Mazloomy Mahmoodabad et al. using POMA on 200 elderly people in Urmia City, Iran, showed that visual impairment was among the diseases that increased the imbalance disorder by 1.7 times [26]. Adequate visual function is important to maintain balance, as it can help people identify and prevent hazards in their environment [32]. On the other hand, visual impairment due to cataracts, glaucoma, macular degeneration, and not wearing glasses can affect one’s ability to move [33]. Balance control is strongly affected by visual motion signals, they provide direct information about head movements [34]. Given the strong relationship between visual impairment and balance control, visual impairment can decrease balance control and increase the risk of falls. But from a sociological point of view, this difference can be due to not wearing glasses as a result of the elderly’s attitude toward glasses or feeling weak and powerless, or on the other hand, due to the feeling of embarrassment or shame for wearing glasses in front of the people around them.
The present study found that women were 2.6 times more likely to fall than men, which is consistent with the results of some studies indicating women have a higher imbalance disorder than men [35-40]. However, some studies have reported no gender difference in balance status [41]. Accordingly, the differences observed in studies could be attributed to the increased life expectancy of women compared to men, different measuring tools for assessing the risk of falls, the health status of participants and the sample size of the participants.
Consistent with the results of the present study, the study by Valipour Dehnou et al. reported that the rate of balance reduction in female elderly was significantly higher than in male elderly (15.79% vs 55.14%) [36]. A study by Azidah et al. on 288 diabetic elderly people showed that the risk of falls was greater in female elderly [35]. This gender-based difference may be attributed to changes in women after menopause and the aging process. Hormonal changes in women may result in osteoporosis, osteoarthritis, muscle weakness, and a faster aging course that can justify less balance in women than men. Moreover, low quality of life for women is considered as the cause of poor balance in female elderly [42]. On the other hand, due to the participation of rural women in difficult activities, such as farming and -livestock activities, it seems that they are more likely to be at risk of fall and balance reduction.
In this study, the probability of falls was 15% higher in the elderly as they get older, which is consistent with some studies [43-45]. However, in some Studies did not show a significant difference in the balance between in some age group of older adults [46]. Natural aging is associated with a decreased ability to maintain balance. Balance maintenance relies on integrating and coordinating the body systems, including sensory, motion, auditory, visual and adaptive components. When the body systems become vulnerable, balance reduces, since they are exposed to degenerative, infectious and traumatic processes. Although mild changes in each aspect of the balance system may not lead to significant perturbation, several component conflicts can lead to a severe decrease in balance in the elderly [47]. Other factors including diabetes, arthritis, hypertension, hearing impairment and marital status were not significantly correlated with balance status in this study, which is not in line with other studies. Differences in the results of different studies can be due to demographic characteristics (rural or urban residency), the number of participants, different lifestyles, habits, and cultures in different communities, the health status of the study participants, and different measurement tools for balance.
Conclusion
This study showed a significant effect of visual impairment, gender, and age factors on balance status and risk of falls in the elderly in rural areas after adjusting for the possible effect of confounding factors. Rural female elderly had a lower balance status than rural male elderly. The results emphasize that healthcare workers should provide more health education in the field of fall prevention to the rural elderly. Moreover, their education should be based on changes in the attitude of the elderly in using assistive devices, such as glasses to prevent falls in the group. Therefore, intervention protocols and prevention methods should be developed to help people who are at risk of falls.
Study strengths and limitations
The strength of the study is the community-based nature of the study and high response rates. The present study is among studies that have examined the balance and risk of falls in the rural elderly population.
However, in the present study, other factors related to balance, such as physical activity and physical and mental health (Alzheimer’s and other cognitive problems) were not assessed. Meanwhile, the type of the elderly’s previous occupation and their work history were not examined and this study did not have an urban group to compare some parameters.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of the Shahid Sadoughi University of Medical Sciences (Code: IR.SSU.SPH.REC.1397.145). The principle of confidentiality and anonymity of the questionnaires was respected and the completion of the questionnaires was done in such a way that it was not boring for the elderly and did not cause any harm to them. Informed consent was obtained orally from the elderly participating in the study. Furthermore, oral consent was received from all participants to enter the study. The completed questionnaire and checklist were anonymous and participants were assured that all information supplied would be kept confidential.
Funding
This study was financially supported by the Shahid Sadoughi University of Medical Sciences.
Authors contributions
Conceptualization and study design: Masoumeh Abbasi-Shavazi, Hosseinali Sadeghian and Sara Jambarsang; Data analysis, data interpretatio and writing the original draft: Masoumeh Abbasi-Shavazi, Sara Jambarsang and Zainab Anbari-Nogyni; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers of this study would like to thank Mohammad Ali Morowati Sharif Abad for his constructive scientific recommendations in the study design and methodology. The authors are also grateful to Mehdi Mohammadi, Vahid Dehghanizadeh Baghdadabad, Hadi Forqani Elahabadi, Ahmed Zare and Hamidah Molanouri Shamsi, Fahima Abedi and Zainab Al-Sadat Hosseini for helping to collect data in this study. The participation of the elderly in this study is also appreciated.
References
According to the forecasts of the current statistics, the world’s elderly population in 2030 will grow from 9% to 16% and in Iran from 6.5% to 17.5% [1]. Evidence suggests that increasing age is strongly associated with functional disorders [2], decreased muscle strength, neural function, physiological function [3] and decreased balance [4]. Also, elderly people are exposed to various diseases because of physiological and pathological changes [5]. Balance and gait disorders are the most common causes of falls in the elderly [6] and the changes in gait in the elderly are often related to underlying conditions, such as illness, especially, increased severity of illness [7]. The prevalence of falls among the elderly was also reported at 27.6%, 30.0%, and 46.8% in other studies [8, 9, 10].
Maintaining balance is a physiological process [3], an essential skill in avoiding falls [7] and an indispensable factor for active participation and contribution to the community [11]. Falls in the elderly population are a major public health problem because they lead to premature mortality and individuals who survive sustain significant losses to their quality of life [12]. Falls can limit daily activities and cause syndromes, such as dependence, immobility and depressive disorder [13]. The results of some studies showed that the increase in age and associated diseases decrease the average score of physical activity in the elderly population [14].
In addition to physical injuries, recurrent falls can have a significant psychological impact. Fear of falling again (post-fall syndrome) can lead elderly individuals to become so afraid of moving that they restrict their activity levels [15]. Some studies have reported risk factors related to imbalance, including diabetes, arthritis, mental disorder [16], falling and reflex, pain, power loss [17], delirium, dementia, Parkinson disease, vitamin B12 deficiency, obesity and stroke [6]. Some other studies in Iran considered factors, such as gender, daily living activity, physical activity, number of diseases and quadriceps muscle strength as the causes of imbalances [20].
The fall accounts for one of the most important factors affecting the onset of functional disorders [21], causing many problems, including increased possibility of falls, reduced independence [11], increased health care needs and level of mortality rates and reduced quality of life related to movement limitation in older people [20]. According to the Iranian elderly health survey in 2015-2016, about 40% of the elderly have gait disorders and 33% use assistive devices. This study also showed that 60% of the elderly were completely dependent on daily activities and 54% had balance disorders [16]. The rural elderly are more at risk compared to urban elderly people due to various aspects, such as education, economic status and health care access. These aspects highlight the importance of studying the balanced status of the rural elderly [19].
Considering the increasing number of elderly and the high prevalence of movement disorders, the risk of falls, and disability in this age group, it is necessary to study the balance in the elderly. On the other hand, the information related to the epidemiology of falls and related factors in rural elderly is limited; therefore, fall risk assessment of the elderly and identifying the major risk factors in this population can provide the appropriate context for practical planning to prevent falls and subsequent disabilities. Accordingly, this study evaluates the balance status and identifies risk factors in the rural elderly of Yazd Province, Iran.
Materials and Methods
Study participants
This cross-sectional study was conducted in rural areas of Yazd Province, Iran, using multi-stage sampling. The participants included 302 elderly people aged over 60 years, considering d=0.6 and s=5.06 (obtained from the pilot study), a power of 80% and an attrition rate of 10%. Firstly, four cities out of 12 cities in Yazd Province, Iran, were randomly selected and one rural healthcare center was selected for sampling in each city. Since the elderly in Iran are provided with inclusive healthcare services and are under healthcare coverage, after listing the names of the elderly covered in the selected rural health centers in each city, approximately 75 people were selected from each center using the systematic random sampling method and invited to participate in the study. The inclusion criteria were the ability to communicate, not taking more than two drugs at the same time in the past 24 h, no dizziness and headache during testing, no psychotropic medication, appropriate diastolic and systolic blood pressure, a lack of severe cognitive disabilities or dementia and the ability to understand verbal instructions. The criteria were identified based on the clinical records of the elderly and their reports.
Data collection instruments
In this study, a multi-section questionnaire, including demographic questions (age, gender, education, tobacco use, history of illness and falls) as well as a questionnaire for assessing gait and balance in the elderly named Tinetti performance oriented mobility assessment (POMA) was used. POMA is an easy adjunctive test that measures gait and balance in the elderly during daily activities. Tinetti gait and balance scale is a reliable and clinically valid tool [21] And It may be a more useful measure than BBS or TUG in patients with impaired dynamic balance or reactive balance during walking [22]. It is one of the best options for assessing the risk of mobility disorders in the elderly [23]. It takes 10 to 15 min and provides the patients with the ability to perform a specific task. Initial scoring tools are performed on three sequential ratings of 0 to 2. A score of 0 indicates a high defect, while a score of 2 indicates the patient’s independence. Each score is a combination of three measures, including gait, balance assessment score and total score. The maximum score is 12 for gait, the maximum for balance is 16, and the total score is 28. Overall, a score below 19 is regarded as a high risk of falls, a score between 19 and 23 identifies a moderate risk, and a score of 24 or higher indicates a low fall risk [24, 25]. The psychometric characteristics of this tool were evaluated and approved in the previous study by Mazloomy Mahmoodabad et al. conducted on Iranian elderly [26]. The questionnaire was completed by trained interviewers who were among the healthcare providers. The subjects were invited to the healthcare center and the questionnaire and checklist were completed for them in a safe place of the healthcare center.
Statistical analysis
Statistical analysis was performed using the SPSS software, version 20. Frequency distribution, Mean±SD were calculated after the normality test using the Kolmogorov-Smirnov test. A chi-square test was used to compare the qualitative variables. Also, the relationship between significant variables with the risk of falls was measured using the ordinal logistic regression model based on the chi-square test. The statistical significance level of P<0.05 was considered in all tests.
Results
This study included 302 elderly people with a mean age of 75.08±6.72 years, most of whom (54%) were aged between 70 and 80 years. Also, 189(62.6%) of the participants were illiterate and 162(54.6%) were female. The percentages of hypertension, arthritis, vision disorders and diabetes were 175(57.9%), 170(56.3%), 99(32.8%) and 87(28.8%), respectively (Table 1).
Table 2 shows the distribution of the participants risk of falls by demographic and disease information.
In terms of risk of falls, 115(38.1%) of the participants were in the high-risk group, 62(20.5%) in the medium-risk group, and 125(41.4%) in the low-risk group. According to the results of the X2 test, the risk of falls was significantly related to gender. Most female subjects (46.9%) were at high fall risk and most male subjects (52.9%) were at low fall risk. Also, 54.5% and 51.5% of the subjects with hearing and visual impairment were at high fall risk, respectively. On the other hand, 45.9% of arthritis patients and 44% of hypertensive patients were at high fall risk. In addition, 51.5% and 71.2% of the elderly, lonely, and elderly aged over 80 years were at high fall risk, respectively (P<0.05).
The odds ratio (OR) with a 95% confidence interval (CI) for investigating the association of the risk of falls with some variables is shown in Table 3.
According to the chi-square table, the variables with P<0.3 were included in the ordinal logistic regression model. Based on the ordinal logistic model, the relationship between significant variables with moderating effects of other variables (gender, marital status, visual and auditory impairments, history of falls, hypertension and arthritis) on the risk of falls was investigated. The results showed that gender, age and visual status had a significant effect on the risk of falls in the elderly (P<0.05). The probability of falls in women was 2.6 times higher than in men. Also, the probability of falls in people with visual impairment was 1.7 times higher than those with no visual impairment. In addition, the probability of falls was 15% higher in the elderly as they get older.
Discussion
This study investigated the balance and factors affecting the risk of falls in the elderly population in Yazd Province, Iran. The results showed that 38.1% of the subjects presented a high fall risk, 20.5% were medium risk and 41.4% showed a low fall risk. The study in Riyadh, Saudi Arabia, showed that 44.5% of people were at high risk of falls, 32.8% were at moderate to severe risk of falls and 22.7% were not at risk of falls [27], which is not in line with the present study. On the other hand, the study by Zarepour in Urmia City, Iran, reported that 47.1%, 42.9% and 10% of the elderly had a severe, moderate and low risk of falls, respectively [28]. A study on the elderly, using the Berg instrument showed that 7.5% of the participants were at moderate or severe and 92.5% were at low risk of fall [29]. The observed differences in the results of surveys on the risk of falls can be explained by differences in the characteristics of participants (urban or rural, different age groups, health conditions), measurement tools for risk assessment of falls, and sample size of participants.
The results showed a significant relationship between visual impairment and the risk of falls in the elderly, which is consistent with previous studies [25, 30, 31]. In the cross-sectional study by Aartolahti et al. on the elderly aged over 76 years, people with poor visual function had significantly lower balance and mobility compared to those with moderate or good visual function [25]. Similarly, the study by Mazloomy Mahmoodabad et al. using POMA on 200 elderly people in Urmia City, Iran, showed that visual impairment was among the diseases that increased the imbalance disorder by 1.7 times [26]. Adequate visual function is important to maintain balance, as it can help people identify and prevent hazards in their environment [32]. On the other hand, visual impairment due to cataracts, glaucoma, macular degeneration, and not wearing glasses can affect one’s ability to move [33]. Balance control is strongly affected by visual motion signals, they provide direct information about head movements [34]. Given the strong relationship between visual impairment and balance control, visual impairment can decrease balance control and increase the risk of falls. But from a sociological point of view, this difference can be due to not wearing glasses as a result of the elderly’s attitude toward glasses or feeling weak and powerless, or on the other hand, due to the feeling of embarrassment or shame for wearing glasses in front of the people around them.
The present study found that women were 2.6 times more likely to fall than men, which is consistent with the results of some studies indicating women have a higher imbalance disorder than men [35-40]. However, some studies have reported no gender difference in balance status [41]. Accordingly, the differences observed in studies could be attributed to the increased life expectancy of women compared to men, different measuring tools for assessing the risk of falls, the health status of participants and the sample size of the participants.
Consistent with the results of the present study, the study by Valipour Dehnou et al. reported that the rate of balance reduction in female elderly was significantly higher than in male elderly (15.79% vs 55.14%) [36]. A study by Azidah et al. on 288 diabetic elderly people showed that the risk of falls was greater in female elderly [35]. This gender-based difference may be attributed to changes in women after menopause and the aging process. Hormonal changes in women may result in osteoporosis, osteoarthritis, muscle weakness, and a faster aging course that can justify less balance in women than men. Moreover, low quality of life for women is considered as the cause of poor balance in female elderly [42]. On the other hand, due to the participation of rural women in difficult activities, such as farming and -livestock activities, it seems that they are more likely to be at risk of fall and balance reduction.
In this study, the probability of falls was 15% higher in the elderly as they get older, which is consistent with some studies [43-45]. However, in some Studies did not show a significant difference in the balance between in some age group of older adults [46]. Natural aging is associated with a decreased ability to maintain balance. Balance maintenance relies on integrating and coordinating the body systems, including sensory, motion, auditory, visual and adaptive components. When the body systems become vulnerable, balance reduces, since they are exposed to degenerative, infectious and traumatic processes. Although mild changes in each aspect of the balance system may not lead to significant perturbation, several component conflicts can lead to a severe decrease in balance in the elderly [47]. Other factors including diabetes, arthritis, hypertension, hearing impairment and marital status were not significantly correlated with balance status in this study, which is not in line with other studies. Differences in the results of different studies can be due to demographic characteristics (rural or urban residency), the number of participants, different lifestyles, habits, and cultures in different communities, the health status of the study participants, and different measurement tools for balance.
Conclusion
This study showed a significant effect of visual impairment, gender, and age factors on balance status and risk of falls in the elderly in rural areas after adjusting for the possible effect of confounding factors. Rural female elderly had a lower balance status than rural male elderly. The results emphasize that healthcare workers should provide more health education in the field of fall prevention to the rural elderly. Moreover, their education should be based on changes in the attitude of the elderly in using assistive devices, such as glasses to prevent falls in the group. Therefore, intervention protocols and prevention methods should be developed to help people who are at risk of falls.
Study strengths and limitations
The strength of the study is the community-based nature of the study and high response rates. The present study is among studies that have examined the balance and risk of falls in the rural elderly population.
However, in the present study, other factors related to balance, such as physical activity and physical and mental health (Alzheimer’s and other cognitive problems) were not assessed. Meanwhile, the type of the elderly’s previous occupation and their work history were not examined and this study did not have an urban group to compare some parameters.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of the Shahid Sadoughi University of Medical Sciences (Code: IR.SSU.SPH.REC.1397.145). The principle of confidentiality and anonymity of the questionnaires was respected and the completion of the questionnaires was done in such a way that it was not boring for the elderly and did not cause any harm to them. Informed consent was obtained orally from the elderly participating in the study. Furthermore, oral consent was received from all participants to enter the study. The completed questionnaire and checklist were anonymous and participants were assured that all information supplied would be kept confidential.
Funding
This study was financially supported by the Shahid Sadoughi University of Medical Sciences.
Authors contributions
Conceptualization and study design: Masoumeh Abbasi-Shavazi, Hosseinali Sadeghian and Sara Jambarsang; Data analysis, data interpretatio and writing the original draft: Masoumeh Abbasi-Shavazi, Sara Jambarsang and Zainab Anbari-Nogyni; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers of this study would like to thank Mohammad Ali Morowati Sharif Abad for his constructive scientific recommendations in the study design and methodology. The authors are also grateful to Mehdi Mohammadi, Vahid Dehghanizadeh Baghdadabad, Hadi Forqani Elahabadi, Ahmed Zare and Hamidah Molanouri Shamsi, Fahima Abedi and Zainab Al-Sadat Hosseini for helping to collect data in this study. The participation of the elderly in this study is also appreciated.
References
- Khezri Moghadam N, Vahidi S, Ashormahani M. [Efficiency of cognitive-existential group therapy on life expectancy and depression of elderly residing in nursing home (Persian)]. Salmand: Iranian Journal of Ageing. 2018; 13(1):62-73. [DOI:10.21859/sija.13.1.62]
- Itakura S, Miyata M, Kuroda A, Setoguchi M, Kusumoto A, Hokonohara D, et al. The association of bite instability and comorbidities in elderly people. Internal Medicine. 2018; 57(11):1569-76. [DOI:10.2169/internalmedicine.9830-17] [PMID]
- Kashani VO, Salmanzade M, Bahrami L. Salmanzade, and L. [Bahrami, Determination of validity and reliability of the Persian version of the 9-item Berg Balance Scale in elderly people (Persian)]. Koomesh. 2018; 20(1):25-33. [Link]
- Hajinia M, Delbari A, Zareii M, Ali abadi M, Habibi A, et al. [Comparison of static balance in active and inactive adult and elderly men (Persian)]. Salmand: Iranian Journal of Ageing. 2013; 8(1):41-8. [Link]
- Papi S, Hosseini S V, Bahadori F, Rezapour V, Moghadasi A M, FadayeVatan R. Oral problems and psychological status of older adults referred to hospital and its relationship with cognition status, stress, anxiety, and depression. Iranian Journal of Health Sciences. 2022; 10(4):19-26. [DOI:10.32598/ijhs.10.4.909.1]
- Cuevas-Trisan R. Balance problems and fall risks in the elderly. Clinics in Geriatric Medicine. 2019; 35(2):173-83. [DOI:10.1016/j.cger.2019.01.008] [PMID]
- Sibley KM, Beauchamp MK, Van Ooteghem K, Straus SE, Jaglal SB. Using the systems framework for postural control to analyze the components of balance evaluated in standardized balance measures: A scoping review. Archives of Physical Medicine and Rehabilitation. 2015; 96(1):122-32. e29. [DOI:10.1016/j.apmr.2014.06.021] [PMID]
- Geetha J, Sakthivadivel V, Gaur A. Assessment of fall risk in elderly rural population. MAEDICA – A Journal of Clinical Medicine. 2021; 16(4):609-14. [DOI:10.26574/maedica.2021.16.4.609]
- Zhang H, Zhao Y, Wei F, Han M, Chen J, Peng S, et al. Prevalence and risk factors for fall among rural elderly: A county-based cross-sectional survey. International Journal of Clinical Practice. 2022; 2022:8042915. [DOI:10.1155/2022/8042915] [PMID]
- Bhoomika V, Chandrappa M, Reddy MM. Prevalence of fall and associated risk factors among the elderly living in a rural area of Kolar. Journal of Family Medicine and Primary Care. 2022; 11(7):3956-60. [DOI:10.4103/jfmpc.jfmpc_1580_21] [PMID]
- Jafari M, Shamshiri M. Reviewing the static and dynamic balance in predicting the risk of falls in elderly people in Tehran. Nursing and Midwifery Faculty. 2015; 12(11):1045-53. [Link]
- Park SH. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clinical and Experimental Research. 2018; 30(1):1-16. [DOI:10.1007/s40520-017-0749-0] [PMID]
- Centre for Health Promotion, Public Health Agency of Canada; British Columbia Injury Research and Prevention Unit (BCIRPU). National fall prevention workshop: Stepping up pan-Canadian coordination. ARCHIVED - Chronic Diseases and Injuries in Canada. 2012; 32(4):227-8. [DOI:10.24095/hpcdp.32.4.07]
- Safarpour M, Hosseini SR, Fotouhi A, Zeraati H, Mohamadzade M, Bijani A. physical activity in the elderly with fall experience over the past year: Results from amirkola health and ageing project. Iranian Journal of Health Sciences. 2019; 7(1):1-8. [DOI:10.18502/jhs.v7i1.1019]
- Hatch J, Gill-Body KM, Portney LG. Determinants of balance confidence in community-dwelling elderly people. Physical Therapy. 2003; 83(12):1072-9. [DOI:10.1093/ptj/83.12.1072] [PMID]
- Al-Momani M, Al-Momani F, Alghadir AH, Alharethy S, Gabr SA. Factors related to gait and balance deficits in older adults. Clinical Interventions in Aging. 2016; 11:1043-9. [DOI:10.2147/CIA.S112282] [PMID]
- Moylan KC, Binder EF. Falls in older adults: Risk assessment, management and prevention. The American Journal of Medicine. 2007; 120(6):493.e1-6. [DOI:10.1016/j.amjmed.2006.07.022] [PMID]
- Cuevas-Trisan R. Balance problems and fall risks in the elderly. Physical Medicine and Rehabilitation Clinics of North America. 2017; 28(4):727-37. [DOI:10.1016/j.pmr.2017.06.006] [PMID]
- Beyranvand R, Sahebozamani M, Daneshjoo A, Seyedjafari E. [Relationship between changes in muscle strength and postural sway after eight weeks aquatic exercise in elderly people: A clinical trial (Persian)]. Journal of Mazandaran University of Medical Sciences. 2018; 27(157):92-104. [Link]
- Shyu ML, Huang HC, Wu MJ, Chang HJ. Development and validation of the self-awareness of falls in Elderly Scale among elderly inpatients. Clinical Nursing Research. 2018; 27(1):105-20. [DOI:10.1177/1054773817714663]
- Curcio F, Basile C, Liguori I, Della-Morte D, Gargiulo G, Galizia G, et al. Tinetti mobility test is related to muscle mass and strength in non-institutionalized elderly people. Age (Dordrecht, Netherlands). 2016; 38(5-6):525-33. [DOI:10.1007/s11357-016-9935-9] [PMID]
- Canbek J, Fulk G, Nof L, Echternach J. Test-retest reliability and construct validity of the tinetti performance-oriented mobility assessment in people with stroke. Journal of Neurologic Physical Therapy. 2013; 37(1):14-9. [DOI: 10.1097/NPT.0b013e318283ffcc] [PMID]
- Köpke S, Meyer G. The Tinetti test: Babylon in geriatric assessment. Zeitschrift fur Gerontologie und Geriatrie. 2006; 39(4):288-91. [DOI:10.1007/s00391-006-0398-y] [PMID]
- Almomani FM, McDowd JM, Bani-Issa W, Almomani M. Health-related quality of life and physical, mental, and cognitive disabilities among nursing home residents in Jordan. Quality of Life Research: An international Journal of Quality of life Aspects of Treatment, Care and Rehabilitation. 2014; 23(1):155-65. [DOI:10.1007/s11136-013-0461-2] [PMID]
- Aartolahti E, Häkkinen A, Lönnroos E, Kautiainen H, Sulkava R, Hartikainen S. Relationship between functional vision and balance and mobility performance in community-dwelling older adults. Aging Clinical and Experimental Research. 2013; 25(5):545-52. [DOI:10.1007/s40520-013-0120-z] [PMID]
- Mazloomy Mahmoodabad SS, Zareipour M, Askarishahi A, Beigomi A. Prevalence of falling and its relation with chronic diseases and balance of older adults in Urmia City. International Journal of Ayurvedic Medicine. 2018; 9(4):273-8. [DOI:10.47552/ijam.v9i4.1114]
- Alshammari SA, Alhassan AM, Aldawsari MA, Bazuhair FO, Alotaibi FK, Aldakhil AA, et al. Falls among elderly and its relation with their health problems and surrounding environmental factors in Riyadh. Journal of Family & Community Medicine. 2018; 25(1):29. [DOI:10.4103/jfcm.JFCM_48_17] [PMID]
- Zarepour M, Jadgal MS, Moradi Z, Movahed E. Assessment of fear of falling and its relation to balance in elderly people of Urmia. Caspian Journal of Health Research. 2020; 5(2):23-7. [DOI:10.29252/cjhr.5.2.23]
- Safarpour M, Hosseini SR, Zeraati H, Bijani A, Fotouhi A. [Balance in the elderly and its determinants (Persian)]. Tehran University Medical Journal. 2018; 76(5):346-53. [Link]
- Dhital A, Pey T, Stanford MR. Visual loss and falls: A review. Eye (London, England). 2010; 24(9):1437-46. [DOI:10.1038/eye.2010.60] [PMID]
- Salive ME, Guralnik J, Glynn RJ, Christen W, Wallace RB, Ostfeld AM. Association of visual impairment with mobility and physical function. Journal of the American Geriatrics Society. 1994; 42(3):287-92. [DOI:10.1111/j.1532-5415.1994.tb01753.x] [PMID]
- Patla AE. Understanding the roles of vision in the control of human locomotion. Gait & Posture. 1997; 5(1):54-69. [DOI:10.1016/S0966-6362(96)01109-5]
- Luxton T, Riglin J. Preventing falls in older people: A multi-agency approach. Nursing Older People (Through 2013). 2003; 15(2):18-21. [DOI:10.7748/nop2003.04.15.2.18.c2249] [PMID]
- Saftari LN, Kwon OS. Ageing vision and falls: A review. Journal of Physiological Anthropology. 2018; 37(1):11. [DOI:10.1186/s40101-018-0170-1] [PMID]
- Azidah AK, Hasniza H, Zunaina E. Prevalence of falls and its associated factors among elderly diabetes in a tertiary center, Malaysia. Current Gerontology and Geriatrics Research. 2012; 2012:539073. [DOI:10.1155/2012/539073] [PMID]
- Valipour Dehnou V, Motamedi R. [Assessing and comparing of balance and flexibility among elderly men and women in the age group of 60-79 years (Persian)]. Salmand: Iranian Journal of Ageing. 2018; 13(2):210-21. [DOI:10.32598/sija.13.2.210]
- Era P, Sainio P, Koskinen S, Haavisto P, Vaara M, Aromaa A. Postural balance in a random sample of 7,979 subjects aged 30 years and over. Gerontology. 2006; 52(4):204-13. [DOI:10.1159/000093652] [PMID]
- Yoshida K, Iwakura H, Inoue F. Motion analysis in the movements of standing up from and sitting down on a chair. A comparison of normal and hemiparetic subjects and the differences of sex and age among the normals. Scandinavian Journal of Rehabilitation Medicine. 1983; 15(3):133-40. [PMID]
- Chacko TV, Thangaraj P, Muhammad GM. Epidemiology of fall and its risk factors among elders in a rural area of Coimbatore, India. International Journal of Community Medicine and Public Health. 2017; 4(10):3864-9. [DOI:10.18203/2394-6040.ijcmph20174265]
- Rekha MR, Mini GK, Kutty VR. Falls among older adults: A community-based study in Rural Kerala, India. Global Journal of Health Science. 2017; 9(10):165. [DOI:10.5539/gjhs.v9n10p165]
- Bryant EC, Trew ME, Bruce AM, Kuisma RM, Smith AW. Gender differences in balance performance at the time of retirement. Clinical Biomechanics (Bristol, Avon). 2005; 20(3):330-5. [DOI:10.1016/j.clinbiomech.2004.11.006] [PMID]
- Taghipour M, Hosseini SR, Pouraria S. [The relationship between physical activity and balance control in the elderly (Persian)]. Salmand: Iranian Journal of Ageing. 2016; 10(4):60-7. [Link]
- Haibach P, Slobounov S, Newell K. Egomotion and vection in young and elderly adults. Gerontology. 2009; 55(6):637-43. [DOI:10.1159/000235816] [PMID]
- Haibach PS, Slobounov SM, Slobounova ES, Newell KM. Aging and time-to-postural stability following a visual perturbation. Aging Clinical and Experimental Research. 2007; 19(6):438-43. [DOI:10.1007/BF03324728] [PMID]
- Amiridis IG, Hatzitaki V, Arabatzi F. Age-induced modifications of static postural control in humans. Neuroscience letters. 2003; 350(3):137-40. [DOI:10.1016/S0304-3940(03)00878-4] [PMID]
- Gomes MM, Reis JG, Neves TM, Petrella M, de Abreu DC. Impact of aging on balance and pattern of muscle activation in elderly women from different age groups. International Journal of Gerontology. 2013; 7(2):106-11. [DOI:10.1016/j.ijge.2012.11.013]
- Matsumura BA, Ambrose AF. Balance in the elderly. Clinics in Geriatric Medicine. 2006; 22(2):395-412; x. [DOI:10.1016/j.cger.2005.12.007] [PMID]
Type of Study: Original Article |
Subject:
Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
