

Volume 12, Issue 2 (Spring 2024)
Iran J Health Sci 2024, 12(2): 149-154 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dehghan O, Azarmi S, Rafinejad J, Moradi-Asl E, Nikookar S H, Akbarzadeh K. Examining A Case Report of Nasopharyngeal Myiasis Caused by Lucilia sericata in Central Iran. Iran J Health Sci 2024; 12 (2) :149-154
URL: http://jhs.mazums.ac.ir/article-1-926-en.html
URL: http://jhs.mazums.ac.ir/article-1-926-en.html
Omid Dehghan * 

 , Sahar Azarmi , Javad Rafinejad , Eslam Moradi-Asl , Seyed Hassan Nikookar , Kamran Akbarzadeh
, Sahar Azarmi , Javad Rafinejad , Eslam Moradi-Asl , Seyed Hassan Nikookar , Kamran Akbarzadeh
, Sahar Azarmi , Javad Rafinejad , Eslam Moradi-Asl , Seyed Hassan Nikookar , Kamran Akbarzadeh
Tropical and Communicable Diseases Research Centre, Iranshahr University of Medical Sciences, Iranshahr, Iran. , omid_dehghan21@yahoo.com
Full-Text [PDF 1383 kb]
(1063 Downloads)
| Abstract (HTML) (2646 Views)
Full-Text: (1274 Views)
Introduction
Myiasis is caused by the laying of eggs of fly larvae on living or dead tissues of the vertebrate hosts. The larvae may attack their hosts through wounds and the natural cavities of the body, including the mouth, ears, eyes, nose, and genitourinary tract [1]. Myiasis is known as a rare human disease and is mainly found in tropical and subtropical areas [2].
Different species of true flies can cause myiasis around the world [3]. The most important flies that cause human myiasis are in four families: Sarcophagidae, Calliphoridae, Muscidae, and Oestridae [4]. In the Calliphoridae family, the genus Lucilia, which is the agent of obligatory myiasis in animals and rarely facultative myiasis in humans, is dispersed worldwide [5]. From 1974 to 2018, about 81 cases of various kinds of myiasis, including wound, nasopharyngeal, auricular, oral, ophthalmic, genitourinary, and intestinal have been reported in Iran, due to clinical and anatomical features, most cases were related to oral myiasis [6]. However, nasal myiasis has been often seen in hospitals, usually caused by Lucilia sericata [7, 8]. Accordingly, this study reports a nasopharyngeal myiasis case caused by L. sericata in a patient with heart and respiratory failure in a hospital in Tehran City, Iran.
Case Presentation
In this study, a 63-year-old man with heart failure and diagnosis of coronary artery and mitral valve replacement referred to a hospital in Tehran. He was treated with long-term antibiotics and steroids for two weeks. The patient was hospitalized for one and a half months in the intensive care unit and had been taken out of the section to get some fresh air during the period of hospitalization. After a while, the physicians noticed the presence of 12 fly larvae in the patient’s nasopharyngeal cavity. The symptoms of myiasis were mild in the patient. After removing all the larvae, the nasal and nasopharyngeal wash was performed with normal saline, and consequently, the symptoms of myiasis disappeared after 48 h and the patient returned to a normal state. Nevertheless, the patient died after 8 days due to severe respiratory and heart failure.
The maggots were transferred to the medical Entomology Laboratory of Tehran University of Medical Sciences for diagnosis and identification. According to the morphological characteristics of the last segment of the larvae body and respiratory organs, the collected specimens from the patient were identified as L. sericata (Figure 1) [9].
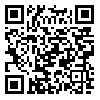
 The last segment of the body of the L. sericata larva has six conical-shaped tubercles around the peritreme and posterior spiracle. The posterior respiratory tract is the most important character for identification of the larvae [9]. The slits which are the entrance holes of the trachea are located obliquely in each spiracle to the center of the larva (Figure 2).
The last segment of the body of the L. sericata larva has six conical-shaped tubercles around the peritreme and posterior spiracle. The posterior respiratory tract is the most important character for identification of the larvae [9]. The slits which are the entrance holes of the trachea are located obliquely in each spiracle to the center of the larva (Figure 2).
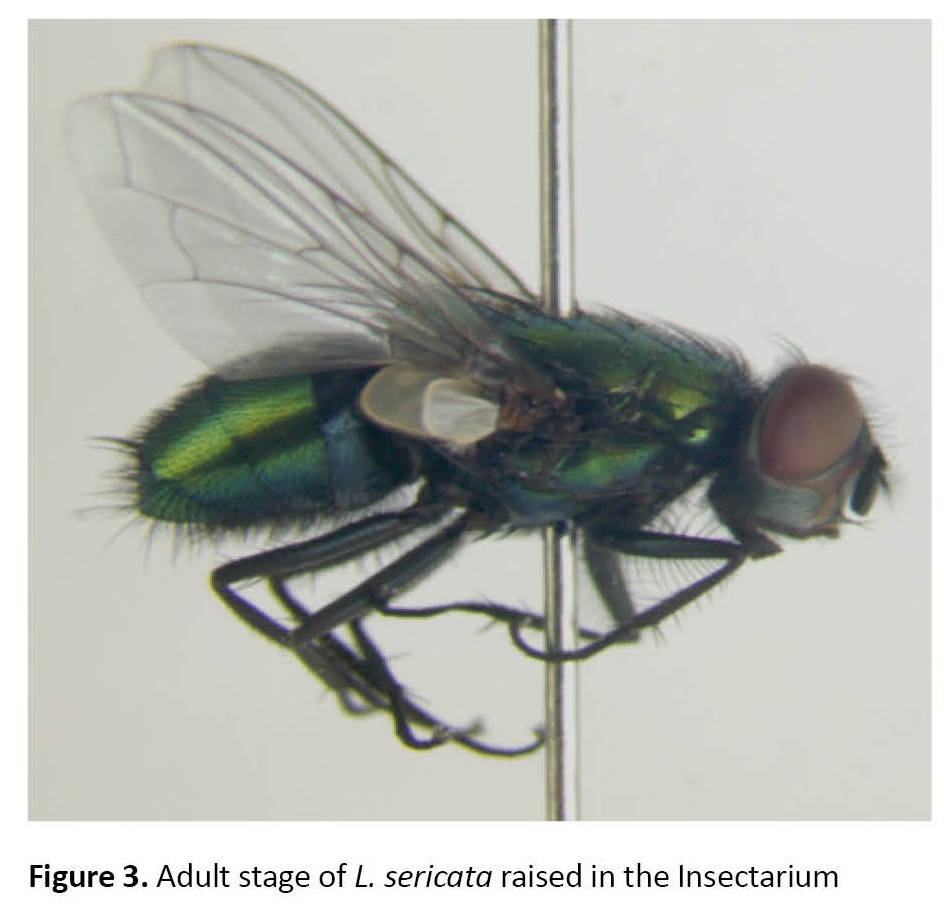
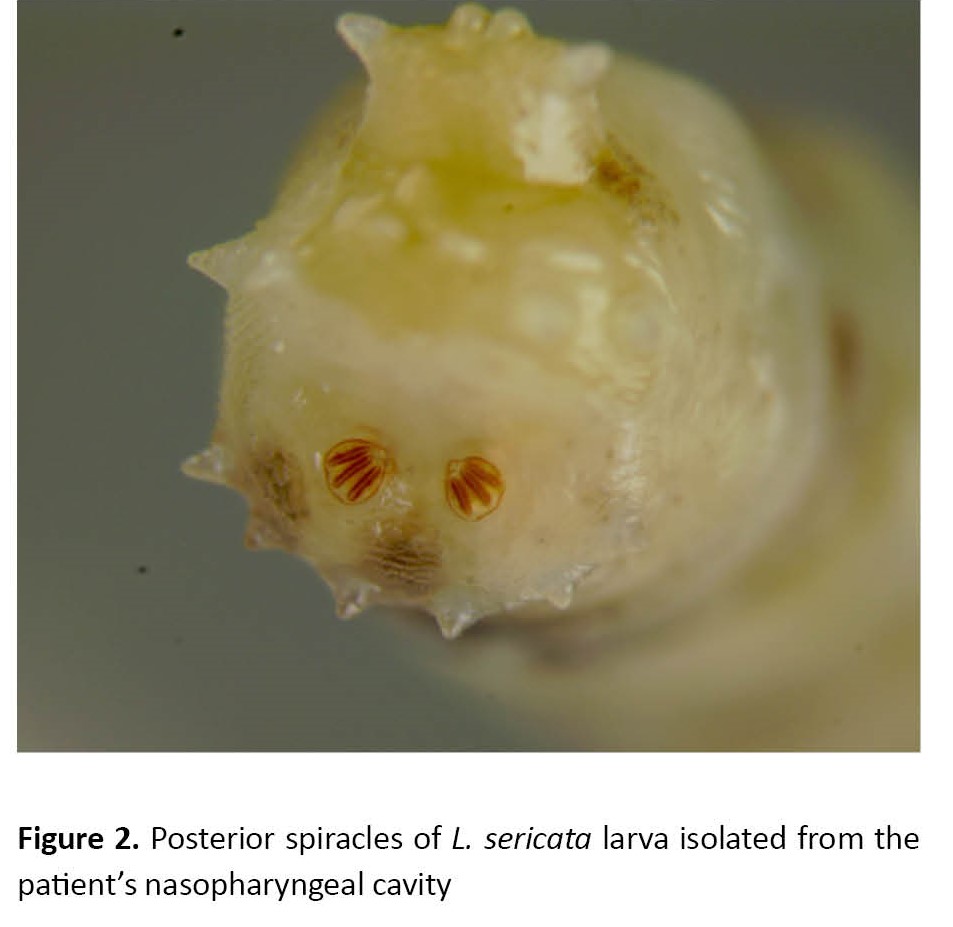 Meanwhile, in the Sarcophagidae larvae, the slits are obliquely outwards or downwards, and in the Muscidae larvae, the slits are sinusoidal or S-shaped [9]. Also, a number of the collected larvae were raised in the Insectarium of the Tehran University of Medical Sciences to become adults, and adult flies were identified as L. sericata using morphological features [10]. During the adult stage, L. sericata has a bright green metallic thorax, hairless lower calypter on the dorsal surface, bright yellow basiocosta, hairless radius vein on the upper surface, the posterior slope of humeral callus with 6–8 hairs, and dark blue front legs (Figure 3) [10].
Meanwhile, in the Sarcophagidae larvae, the slits are obliquely outwards or downwards, and in the Muscidae larvae, the slits are sinusoidal or S-shaped [9]. Also, a number of the collected larvae were raised in the Insectarium of the Tehran University of Medical Sciences to become adults, and adult flies were identified as L. sericata using morphological features [10]. During the adult stage, L. sericata has a bright green metallic thorax, hairless lower calypter on the dorsal surface, bright yellow basiocosta, hairless radius vein on the upper surface, the posterior slope of humeral callus with 6–8 hairs, and dark blue front legs (Figure 3) [10].
Discussion
Nasopharyngeal myiasis is a type of infestation with larvae of various dipterous flies that is often common in tropical and subtropical regions of the world [11]. In the study of Alizadeh et al., the infestation rate for nasal myiasis was reported at around 4% in Iran, most of which were reported from the south of the country, and the proven mortality rate due to nasal myiasis was 1.3% [12]. Due to the lack of a government reporting system for myiasis disease, accurate information on the status of this disease is unavailable in Tehran and most provinces in Iran. Myiasis is classified based on many factors, such as the location of the larva on the host, the causative agents, and the type of host-maggot relationship [1, 13]. Infestation of the host with larvae of dipterous flies occurs once female flies lay their eggs on the necrotic or living tissue of the human or animal body [13]. Various species of flies, such as Chrysomya bezziana, Wohlphartia magnifica, and Oestrus ovis which cause human myiasis have been reported in Iran [6, 14-16].
The most important family that causes myiasis is Calliphoridae, which includes the genera Calliphora, Lucilia, Chrysomia, Cochliomyia, and Phormia [4]. Facultative myiasis agents feed on the living or necrotic tissue of the host body. Flies of the genera Calliphora, Lucilia, and Phormia cause facultative myiasis and their larvae when placed on the open wounds help to create granular tissue, remove bacteria and necrotic tissue, and heal wounds [17]. The agents of obligatory myiasis, such as Chrysomia and Cochliomyia flies need to lay their eggs or larvae on the living tissue of the host to complete their life cycle. In terms of the location of larvae on the host, myiasis is classified as cutaneous, furuncular, gastrointestinal, genitourinary, nasopharyngeal, oral, nasal, auricular, and ophthalmic. The most common type of myiasis is cutaneous myiasis, which occurs in various forms of wound (traumatic), migratory, furuncular, and nodules [18].
Yassin reported a 62-year-old man with wound myiasis in Iran in which the myiasis agent was the larvae of L. sericata as in the present study [19]. Nosocomial myiasis is a rare phenomenon in hospitalized patients [20 ]. The physical weakness of patients, lack of hygiene, open wounds without dressing, wound bleeding, necrotic tissues, decomposition odor, and inattention to proper nursing care are some predisposing factors for nosocomial myiasis [21]. In patients with myiasis, secondary bacterial and fungal infections may occur and this can be dangerous in patients with weakened immune systems [22].
Most myiasis, especially nasopharyngeal, oral, and nasal, is due to poor hygiene sleeping with the mouth open, and consequently laying eggs by flies inside the mouth. The most appropriate way to prevent flies is to maintain good personal hygiene, manage food waste, collect and dispose of garbage on time, cover wounds, and use window nets and repellents. Moreover, the use of electric indoor fly traps and bait traps can reduce the population of flies. Also, if the abundance of flies is high, insecticides with knock-down effects, such as resmethrin, can be used in the forms of spraying and fogging. It is recommended that measures be taken to prevent insects including flies from entering hospitals and control them [6, 23, 24]. Ivermectin is also used as a drug in veterinary medicine to kill various ectoparasites and endoparasites of livestock [25]. Therefore, ivermectin can be used to destroy fly larvae in livestock and control their population in rural areas.
Conclusion
It is important to educate hospital staff about myiasis and the role of flies in disease transmission, along with planning to design appropriate control measures for flies in the hospital environment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iranshahr University of Medical Sciences (Code: IR.IRSHUMS.REC.1402.017).
Funding
This research was supported by the research project (No.: IR.IRSHUMS.REC.1402.017), Funded by the Iranshahr University of Medical Sciences.
Authors contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors express their gratitude to all who contributed to the research process.
References
Myiasis is caused by the laying of eggs of fly larvae on living or dead tissues of the vertebrate hosts. The larvae may attack their hosts through wounds and the natural cavities of the body, including the mouth, ears, eyes, nose, and genitourinary tract [1]. Myiasis is known as a rare human disease and is mainly found in tropical and subtropical areas [2].
Different species of true flies can cause myiasis around the world [3]. The most important flies that cause human myiasis are in four families: Sarcophagidae, Calliphoridae, Muscidae, and Oestridae [4]. In the Calliphoridae family, the genus Lucilia, which is the agent of obligatory myiasis in animals and rarely facultative myiasis in humans, is dispersed worldwide [5]. From 1974 to 2018, about 81 cases of various kinds of myiasis, including wound, nasopharyngeal, auricular, oral, ophthalmic, genitourinary, and intestinal have been reported in Iran, due to clinical and anatomical features, most cases were related to oral myiasis [6]. However, nasal myiasis has been often seen in hospitals, usually caused by Lucilia sericata [7, 8]. Accordingly, this study reports a nasopharyngeal myiasis case caused by L. sericata in a patient with heart and respiratory failure in a hospital in Tehran City, Iran.
Case Presentation
In this study, a 63-year-old man with heart failure and diagnosis of coronary artery and mitral valve replacement referred to a hospital in Tehran. He was treated with long-term antibiotics and steroids for two weeks. The patient was hospitalized for one and a half months in the intensive care unit and had been taken out of the section to get some fresh air during the period of hospitalization. After a while, the physicians noticed the presence of 12 fly larvae in the patient’s nasopharyngeal cavity. The symptoms of myiasis were mild in the patient. After removing all the larvae, the nasal and nasopharyngeal wash was performed with normal saline, and consequently, the symptoms of myiasis disappeared after 48 h and the patient returned to a normal state. Nevertheless, the patient died after 8 days due to severe respiratory and heart failure.
The maggots were transferred to the medical Entomology Laboratory of Tehran University of Medical Sciences for diagnosis and identification. According to the morphological characteristics of the last segment of the larvae body and respiratory organs, the collected specimens from the patient were identified as L. sericata (Figure 1) [9].
Discussion
Nasopharyngeal myiasis is a type of infestation with larvae of various dipterous flies that is often common in tropical and subtropical regions of the world [11]. In the study of Alizadeh et al., the infestation rate for nasal myiasis was reported at around 4% in Iran, most of which were reported from the south of the country, and the proven mortality rate due to nasal myiasis was 1.3% [12]. Due to the lack of a government reporting system for myiasis disease, accurate information on the status of this disease is unavailable in Tehran and most provinces in Iran. Myiasis is classified based on many factors, such as the location of the larva on the host, the causative agents, and the type of host-maggot relationship [1, 13]. Infestation of the host with larvae of dipterous flies occurs once female flies lay their eggs on the necrotic or living tissue of the human or animal body [13]. Various species of flies, such as Chrysomya bezziana, Wohlphartia magnifica, and Oestrus ovis which cause human myiasis have been reported in Iran [6, 14-16].
The most important family that causes myiasis is Calliphoridae, which includes the genera Calliphora, Lucilia, Chrysomia, Cochliomyia, and Phormia [4]. Facultative myiasis agents feed on the living or necrotic tissue of the host body. Flies of the genera Calliphora, Lucilia, and Phormia cause facultative myiasis and their larvae when placed on the open wounds help to create granular tissue, remove bacteria and necrotic tissue, and heal wounds [17]. The agents of obligatory myiasis, such as Chrysomia and Cochliomyia flies need to lay their eggs or larvae on the living tissue of the host to complete their life cycle. In terms of the location of larvae on the host, myiasis is classified as cutaneous, furuncular, gastrointestinal, genitourinary, nasopharyngeal, oral, nasal, auricular, and ophthalmic. The most common type of myiasis is cutaneous myiasis, which occurs in various forms of wound (traumatic), migratory, furuncular, and nodules [18].
Yassin reported a 62-year-old man with wound myiasis in Iran in which the myiasis agent was the larvae of L. sericata as in the present study [19]. Nosocomial myiasis is a rare phenomenon in hospitalized patients [20 ]. The physical weakness of patients, lack of hygiene, open wounds without dressing, wound bleeding, necrotic tissues, decomposition odor, and inattention to proper nursing care are some predisposing factors for nosocomial myiasis [21]. In patients with myiasis, secondary bacterial and fungal infections may occur and this can be dangerous in patients with weakened immune systems [22].
Most myiasis, especially nasopharyngeal, oral, and nasal, is due to poor hygiene sleeping with the mouth open, and consequently laying eggs by flies inside the mouth. The most appropriate way to prevent flies is to maintain good personal hygiene, manage food waste, collect and dispose of garbage on time, cover wounds, and use window nets and repellents. Moreover, the use of electric indoor fly traps and bait traps can reduce the population of flies. Also, if the abundance of flies is high, insecticides with knock-down effects, such as resmethrin, can be used in the forms of spraying and fogging. It is recommended that measures be taken to prevent insects including flies from entering hospitals and control them [6, 23, 24]. Ivermectin is also used as a drug in veterinary medicine to kill various ectoparasites and endoparasites of livestock [25]. Therefore, ivermectin can be used to destroy fly larvae in livestock and control their population in rural areas.
Conclusion
It is important to educate hospital staff about myiasis and the role of flies in disease transmission, along with planning to design appropriate control measures for flies in the hospital environment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iranshahr University of Medical Sciences (Code: IR.IRSHUMS.REC.1402.017).
Funding
This research was supported by the research project (No.: IR.IRSHUMS.REC.1402.017), Funded by the Iranshahr University of Medical Sciences.
Authors contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors express their gratitude to all who contributed to the research process.
References
- Francesconi F, Lupi O. Myiasis. Clinical Microbiology Reviews. 2012; 25(1):79-105. [DOI:10.1128/CMR.00010-11] [PMID] [PMCID]
- Afifi MA, Jiman-Fatani AA, Alsiny FI, Anshasi WS. A new focus of autochthonous transmission of Cordylobia anthropophaga in Saudi Arabia. Journal of Microscopy and Ultrastructure. 2015; 3(2):82-85. [DOI:10.1016/j.jmau.2014.12.002] [PMID] [PMCID]
- Bautista-Garfias CR, Aguilar-Marcelino L, Nogueda-Torres B. Myiasis infections in animals and men. In: Aguilar-Marcelino L, Younus M, Khan A, Saeed NM and Abbas RZ, editors. One health triad. Faisalabad: Unique Scientific Publishers; 2023. [Link]
- Nouri NV, Salehi A. Myiasis in humans and animals. ES Journal of Dental Sciences. 2020; 1(3):1017. [Link]
- Hosni EM, Kenawy MA, Nasser MG, Al-Ashaal SA, Rady MH. A brief review of myiasis with special notes on the blow flies’ producing myiasis (F.: calliphoridae). Egyptian Academic Journal of Biological Science. 2019; 11(2):25-32. [DOI:10.21608/eajbse.2019.52823]
- Hazratian T, Dolatkhah A, Akbarzadeh K, Khosravi M, Ghasemikhah R. A review of human myiasis in Iran with an emphasis on reported cases. Malaysian Journal of Medicine and Health Sciences. 2020; 16(2):269-74. [Link]
- Mowlavi G, Nateghpour M, Teimoori S, Amin A, Noohi F, Kargar F. Fatal nosocomial myiasis caused by Lucilia sericata. The Journal of Hospital Infection. 2011; 78(4):338-9. [DOI:10.1016/j.jhin.2011.04.005] [PMID]
- Maleki Ravasan N, Shayeghi M, Najibi B, Oshaghi MA. Infantile nosocomial myiasis in iran. Journal of Arthropod-Borne Diseases. 2012; 6(2):156-63. [PMID] [PMCID]
- Szpila, K. (2009). Key for the identification of third instars of European blowflies (diptera: Calliphoridae) of forensic importance. In: Amendt J, Goff ML, Campobasso CP, Grassberger M, editors. Current concepts in forensic entomology. Berlin: springer; 2009. [DOI:10.1007/978-1-4020-9684-6_3]
- Akbarzadeh K, Wallman JF, Sulakova H, Szpila K. Species identification of Middle Eastern blowflies (diptera: Calliphoridae) of forensic importance. Parasitology Research. 2015; 114(4):1463-72. [DOI:10.1007/s00436-015-4329-y] [PMID] [PMCID]
- Swain SK, Sahu MC, Baisakh MR. Nasal myiasis in clinical practice. Apollo Medicine. 2018; 15(3): 128-31. [Link]
- Alizadeh M, Mowlavi G, Kargar F, Nateghpour M, Akbarzadeh K, Hajenorouzali-Tehrani M. A review of myiasis in Iran and a new nosocomial case from Tehran, Iran. Journal of Arthropod-Borne Diseases. 2014; 8(2):124-31. [PMID] [PMCID]
- Bernhardt V, Finkelmeier F, Verhoff MA, Amendt J. Myiasis in humans-a global case report evaluation and literature analysis. Parasitology Research. 2019; 118(2):389-97. [DOI:10.1007/s00436-018-6187-x] [PMID]
- Goddard J. Physician’s guide to arthropods of medical importance. Boca Raton: CRC Press, 2016. [DOI:10.1201/b12930]
- Mohammadzadeh T, Hadadzadeh R, Esfandiari F, Sadjjadi S. A case of gingival myiasis caused by Wohlfahrtia magnifica. Iran. Journal of Arthropod-Borne Diseases. 2008; 2(1): 35-6. [Link]
- Mircheraghi SF, Mircheraghi SF, Ramezani Awal Riabi H, Parsapour A. Nasal nosocomial myiasis infection caused by chrysomya bezziana (diptera: Calliphoridae) following the septicemia: A case report. Iranian Journal of Parasitology. 2016; 11(2):284-9. [PMID] [PMCID]
- Dehghan O, Mehdi TS, Rafinejad J, Toutonnchy M, Tiyuri A, Akbarzadeh K, et al;. A new approach to maggot therapy for healing of diabetic foot ulcers. Acta facultatis medicae Naissensis. 2020; 37(4):387-95. [DOI:10.5937/afmnai2004387D]
- Robbins K, Khachemoune A. Cutaneous myiasis: A review of the common types of myiasis. International Journal of Dermatology. 2010; 49(10):1092-8. [DOI:10.1111/j.1365-4632.2010.04577.x] [PMID]
- Yasin M, Gozali Asl N, Mojdehi AM, Mardani M, Akbarzadeh K. Wound myiasis in a sixty-two-year-old man. Archives of Clinical Infectious Diseases. 2014; 9(2):e19659. [DOI:10.5812/archcid.19659]
- Szakacs TA, MacPherson P, Sinclair BJ, Gill BD, McCarthy AE. Nosocomial myiasis in a Canadian intensive care unit. CMAJ. 2007; 177(7):719-20. [DOI:10.1503/cmaj.061598] [PMID] [PMCID]
- Predy G, Angus M, Honish L, E Burnett C, Stagg A. Myiasis in an urban setting: A case report. The Canadian Journal of Infectious Diseases. 2004; 15(1):51-2. [DOI:10.1155/2004/978427] [PMID] [PMCID]
- Mahdy D, Wathah EF. Isolation and diagnosis of the bacteria causing corneal ulceration associated with ocular myiasis infection. Indian Journal of Forensic Medicine & Toxicology. 2022; 16(1):352-7. [DOI:10.37506/ijfmt.v16i1.17479]
- Khoobdel M, Sobati H, Dehghan O, Akbarzadeh K, Radi E. Natural host preferences of parasitoid wasps (hymenoptera: Pteromalidae) on synanthropic flies. European Journal of Translational Myology. 2019; 29(2):8197. [DOI:10.4081/ejtm.2019.8197] [PMID] [PMCID]
- Frye MA. Multisensory systems integration for high-performance motor control in flies. Current Opinion in Neurobiology. 2010; 20(3):347-52. [DOI:10.1016/j.conb.2010.02.002] [PMID] [PMCID]
- Forbes A. Strategic planning for parasite control on livestock farms. Livestock. 2019; 24(2):82-7. [DOI:10.12968/live.2019.24.2.82]
Type of Study: Case Report/Research Letter |
Subject:
Medical Entomology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
