

Volume 12, Issue 2 (Spring 2024)
Iran J Health Sci 2024, 12(2): 89-98 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Karki R, Timsina A, Kaphle M, Sah R. Prevalence and Factors of Social Anxiety Disorder Among Health Science Students in Kathmandu. Iran J Health Sci 2024; 12 (2) :89-98
URL: http://jhs.mazums.ac.ir/article-1-934-en.html
URL: http://jhs.mazums.ac.ir/article-1-934-en.html



Central Department of Public Health, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal. , karkirajesh2022@gmail.com
Full-Text [PDF 779 kb]
(1414 Downloads)
| Abstract (HTML) (3651 Views)
Full-Text: (1735 Views)
Introduction
Social anxiety disorder (SAD), also known as social phobia, is an anxiety disorder characterized by intense discomfort and anxiety related to potential rejection, humiliation, or negative evaluation in social situations [1]. Individuals afflicted by SAD may exhibit non-specific fears in ambiguous situations or specific tasks, such as public speaking or eating in the presence of others [2]. Initially recognized as a significant issue in the 19th century, the prevalence of social anxiety has surged over the 20th and 21st centuries, often referred to as the age of anxiety [3].
According to the World Health Organization (WHO), nearly 301 million individuals, including 58 million children and adolescents, were affected by anxiety disorders globally in 2019 [4]. Research findings suggest that the lifetime prevalence of SAD falls within the range of 3%–13%. Among university students globally, rates fluctuate from 9% to 16.1%, with notably higher rates observed in Ethiopia (26%) and India (31.1%) [5]. Moreover, data from studies across seven countries indicate that the lifetime prevalence of social phobia ranges from 22.9% to 57.6% [6].
SAD often coexists with other mental health conditions, such as eating disorders (comorbidity rates up to 60%) and mood disorders like depression and bipolar disorder (comorbidity rates ranging from 35% to 70% and 3.5% to 21%, respectively [7].
In Nepal, the mental health of adolescents is a major concern, with three-quarters of teenagers reporting anxiety in a nationwide study [8]. A study in the Dang District of Nepal found that nearly half of high school adolescents in grades 9 to 12 were affected by anxiety disorders [9]. Similarly, a study among undergraduate students of management in Kathmandu City, Nepal, revealed a higher prevalence of anxiety compared to stress and depression [10].
University students, who heavily rely on virtual social networks for communication, may be at increased risk for social anxiety due to the potential avoidance of face-to-face interaction [11].
Social anxiety, which disproportionately affects young people, is a rapidly growing phenomenon [12]. In today’s competitive environment, particularly among students, where high academic performance is emphasized, social anxiety disorder has become increasingly significant [13]. However, despite its prevalence, social anxiety disorder often remains underdiagnosed and undertreated [14]. Given the importance of social anxiety as an indicator of adult functioning, there is a dearth of studies evaluating its prevalence and impact specifically among Nepalese teenagers [8]. Therefore, this study investigates the prevalence of social anxiety disorders and identifies associated factors among bachelor-level health science students in Kathmandu City, Nepal.
Materials and Methods
Study design, area, and population
A web-based cross-sectional study was conducted in 2023 among health science students enrolled in bachelor-level programs, specifically bachelor’s degrees in public health, nursing, and post-basis bachelor of nursing, from five selected colleges in Kathmandu City, Nepal.
Sample size determination and sampling technique
The sample size for the study was determined using the formula n=Z2pq/d2, with an assumed prevalence of social phobia symptoms among students (p)=31.2% [15], a Z score of 1.96 for a 95% confidence level, and a desired margin of error (d) of 0.05. This calculation yielded a final sample size of 330. Given the occurrence of student vacations during the data collection period and potential imitations on response rates, we employed the purposive sampling technique. Specifically, we e-mailed all students enrolled in the respective programs at the five selected colleges in Kathmandu City, Nepal.
Data collection
A self-constructed structured questionnaire was used to measure the study objectives and distributed to participants. This questionnaire included three sections. The first section collected sociodemographic information, including age, sex, and relevant background characteristics. The second section explored factors potentially associated with SAD, such as perceived parental behavior, experience of negative life events, perceived individual appearance, and peer relationships. These questions were formulated after an extensive literature review. The third section addressed SAD measurement directly. A validated tool called the social phobia inventory (SPIN) was employed. This self-report questionnaire utilizes a 5-point Likert scale (ranging from “not at all” to “extremely”) for each of its 17 items. The total score on the SPIN ranges from 0 to 68, with higher scores indicating a greater degree of social anxiety [16].
Before data collection, the researchers obtained a list of students and their e-mail addresses from the respective colleges with appropriate permissions. The questionnaire was then e-mailed to all students, accompanied by clear instructions for completion. This approach aimed to maximize the potential participant pool while acknowledging the impact of the vacation period on response rates. The data collection period spanned from March 31st, 2023, to May 14th, 2023. However, due to the strict time frame of our study and the cessation of responses after this date, a total of 325 students actively participated, resulting in a response rate of 98.48%. This comprehensive e-mail distribution to all eligible students ensured that our response rate was maximized given the constraints of the study.
Prevalence of social anxiety disorder
To determine the prevalence of SAD among the participants, we utilized a cut-off score of 19 on SPIN. A score of 19 or higher indicates the presence of social phobia [17]. According to studies, the tool accurately predicts social anxiety in 78% of cases based on this cut-off score [16].
Validation of the questionnaire
The subject expert validated the questionnaire. To assess its reliability, we conducted a pre-testing on 10% of the total sample size within a similar area. The reliability was determined using the Cronbach α method, which yielded a calculated value of 0.95.
Data quality control
All responses were carefully reviewed daily to ensure consistency. The final set of responses was imported into the SPSS software, version 26, for identifying and addressing missing values and outliers. In case of any missing values or outliers, the respective participants were contacted again. Each variable was appropriately coded. All researchers actively participated in this stage of the process.
Data analysis and presentation
The data analysis was conducted using the SPSS software. Descriptive analysis was performed to calculate frequencies, percentages, Mean±SD for the socio-demographic factors and variables related to SAD. To identify the significant predictors of social anxiety disorder, a binary logistic regression model was utilized with a 95% confidence interval. The adjusted odds ratio (AOR) or odds ratio (OR) was estimated to quantify the strength of association between the independent variables (socio-demographic factors, perceived parental behavior, experience of negative life events, perceived individual appearance, peer relations) and the dependent variable (SAD). The statistical significance level was set at P<0.05. The findings included AOR/OR values, confidence intervals, and P for each predictor variable.
Results
Socio-demographic characteristics of the sample
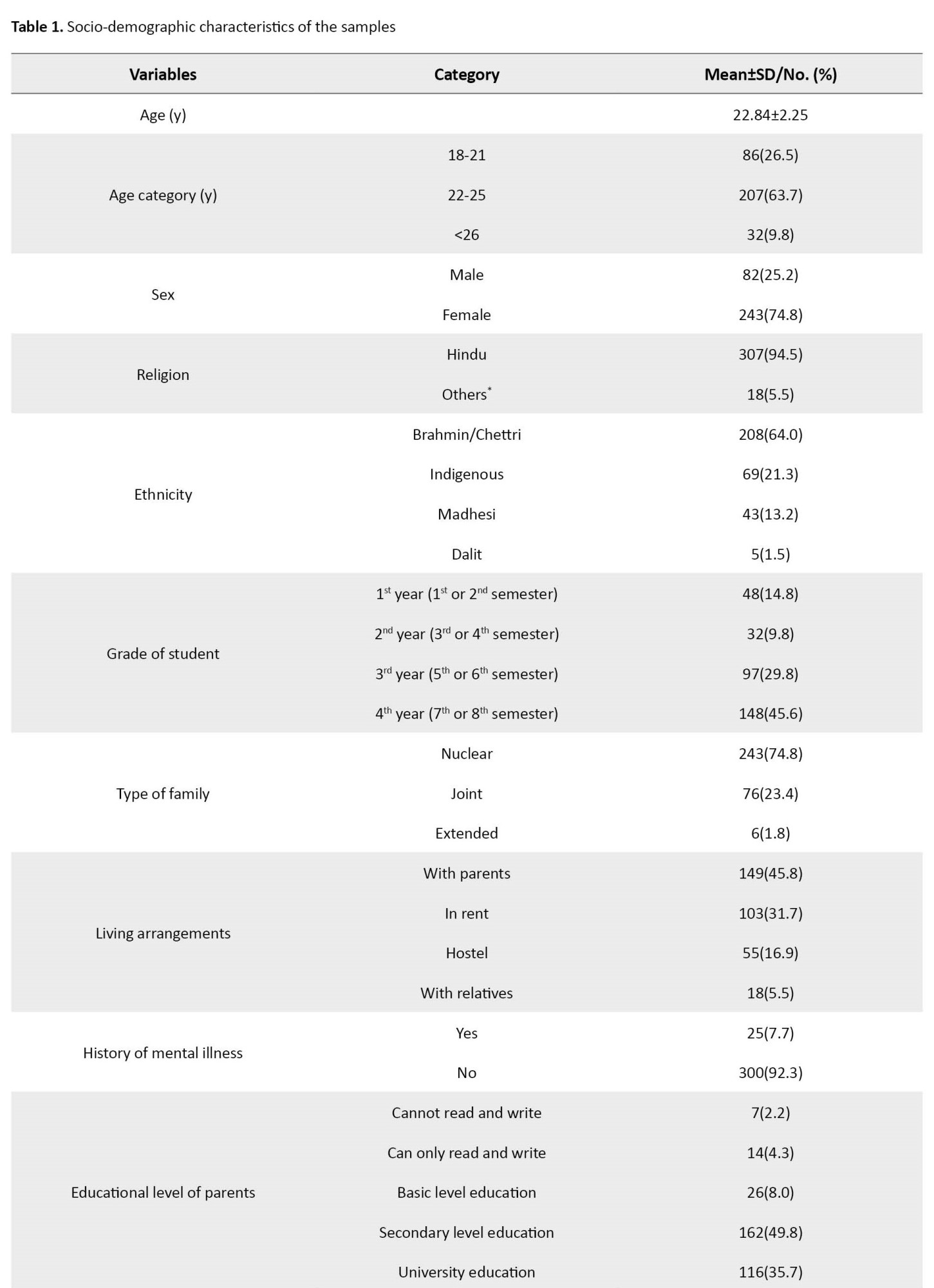
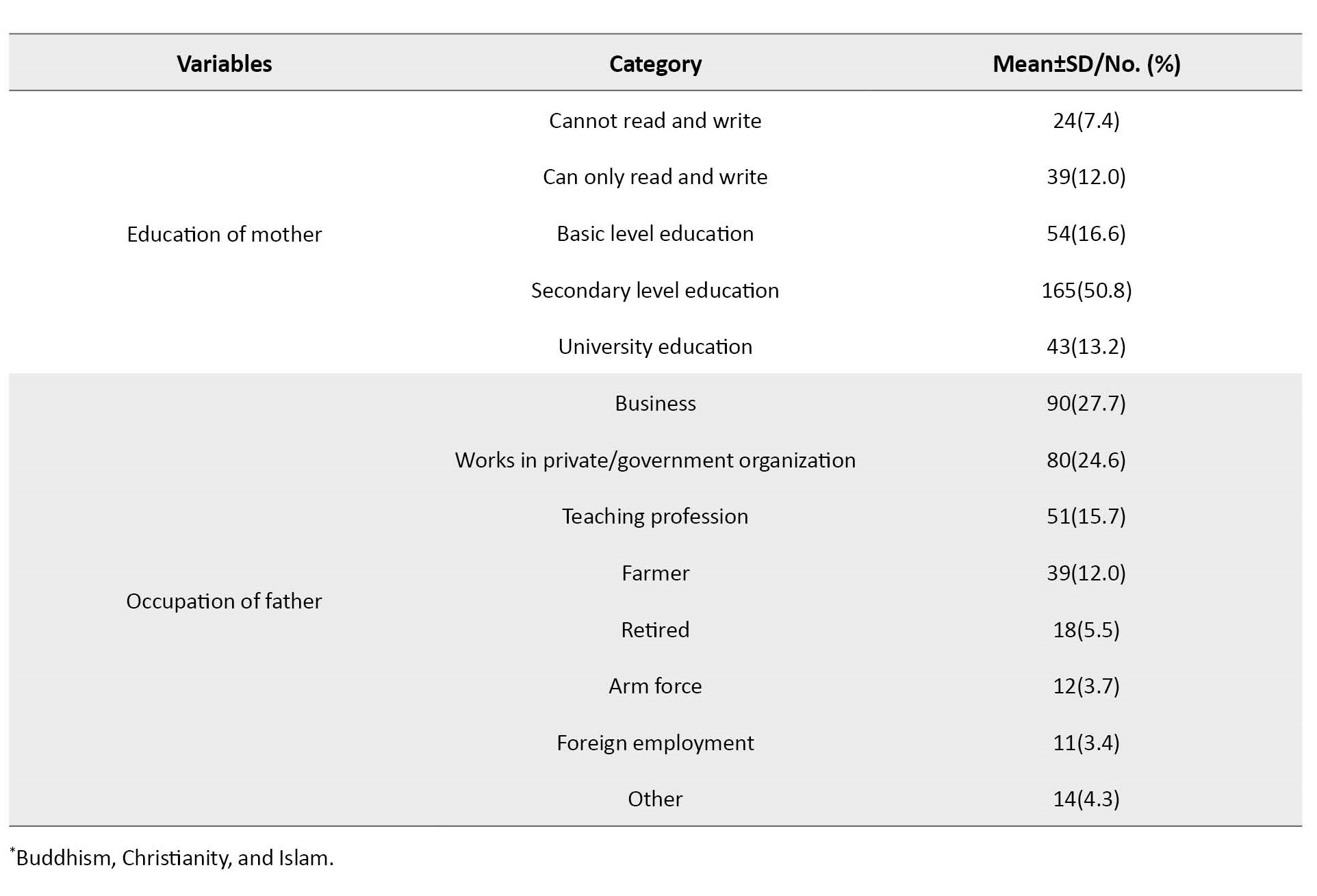
Out of 325 participants, the study included a large portion of young adults aged 22-25 years (63.7%, n=207), with a mean age of 22.84±2.25 years. Females comprised most of the participants (74.8%, n=243). Regarding religion, Hinduism was the most prevalent faith (94.5%, n=307). Brahmin/Chettri emerged as the dominant caste (64.0%, n=208), and nuclear families were the most common family structure (74.8%, n=243). Nearly half (45.8%, n=149) of the participants resided with their parents, while only a small percentage (7.7%, n=25) reported a prior history of mental illness (Table 1).
Perceived parental behavior, experience of negative life events, perceived individual appearance, and peer relations
Perceived parental behavior
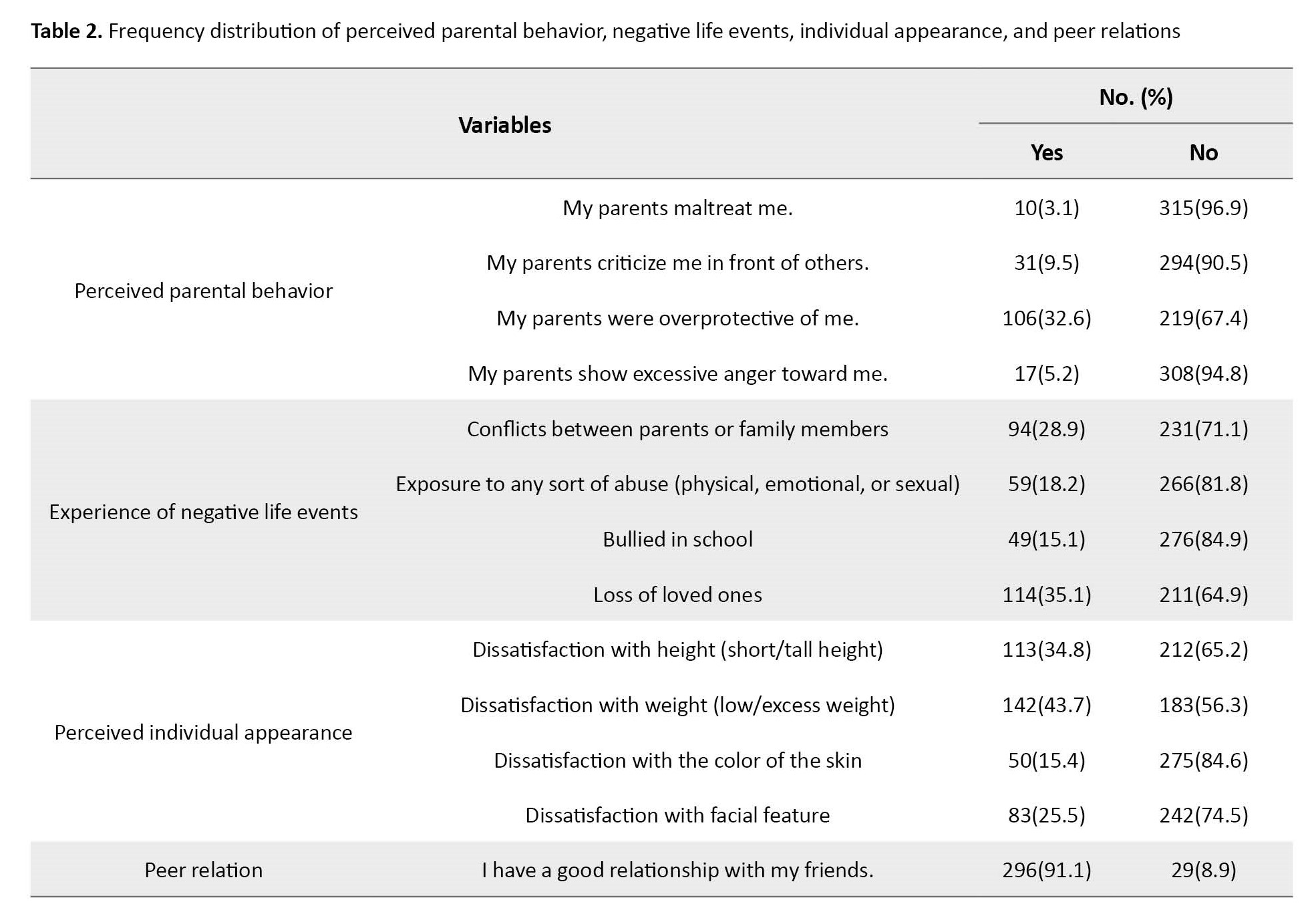
Only 3.1% (n=10) of the participants reported experiencing maltreatment from their parents, while 9.5% (n=31) mentioned that their parents criticized them in front of others. Furthermore, 32% (n=106) of the participants reported that their parents overprotect them, and a small percentage (5.2%, n=17) mentioned experiencing excess anger from their parents.
Experience of negative life events
Approximately 28.9% (n=94) of the participants reported conflicts between their parents or family members, while 18.2% (n=59) mentioned exposure to any sort of abuse. A notable percentage of participants (15.1%) reported being bullied in school, and the loss of loved ones was reported by 35.1% (n=114) of the participants.
Perceived individual appearance
Among the participants, 34.8% (n=113) mentioned dissatisfaction with their height (short/tall height), while 43.7% (n=142) expressed dissatisfaction with their weight (low/excess weight). A small percentage of participants (15.4%, n=50) reported dissatisfaction with the color of their skin, and 25.5% (n=83) mentioned dissatisfaction with their facial features.
Peer relations
The majority of participants (91.1%, n=296) mentioned having a good relationship with their friends, while only a small percentage (8.9%) reported having a poor relationship with their friends (Table 2).
Prevalence and level of social anxiety disorder
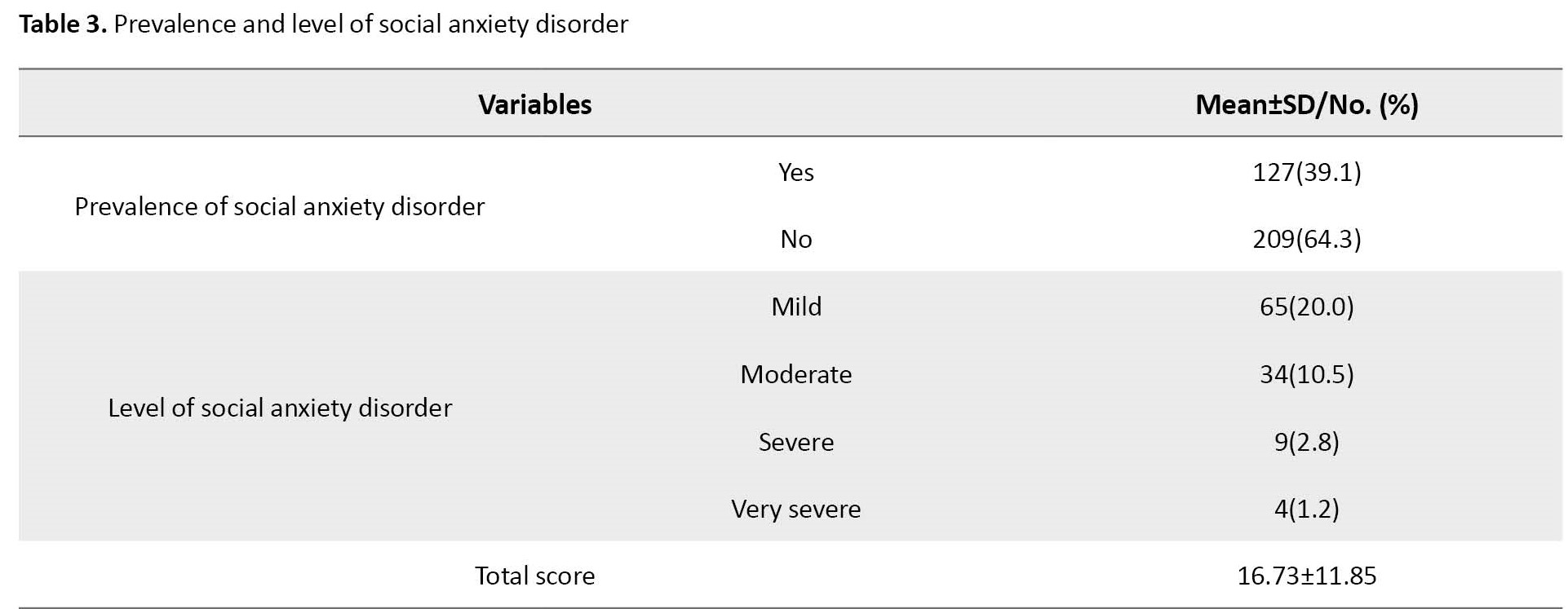
Out of the 325 participants, social anxiety disorder was present among 39.1% (n=127), with a mean score of 16.73±11.85. Categorically, the majority had mild social anxiety disorder (20.0%, n=65), while only 2.8% had severe, and 1.2% had a very severe level of SAD (Table 3).
Logistic regression analysis of factors associated with social anxiety disorder
A logistic regression analysis was performed to assess the association between selected variables and social anxiety disorder. Only variables that showed a significant association with social anxiety disorder were included in the model. The results revealed that the model was statistically significant, as indicated by the Omnibus tests of model coefficients (χ2=62.649, P<0.001). The model showed a good fit to the data, as indicated by the Hosmer and Lemeshow test (χ2=9.354, P=0.313), and a 0.2 Nagelkerke pseudo-R2 (Table 4).
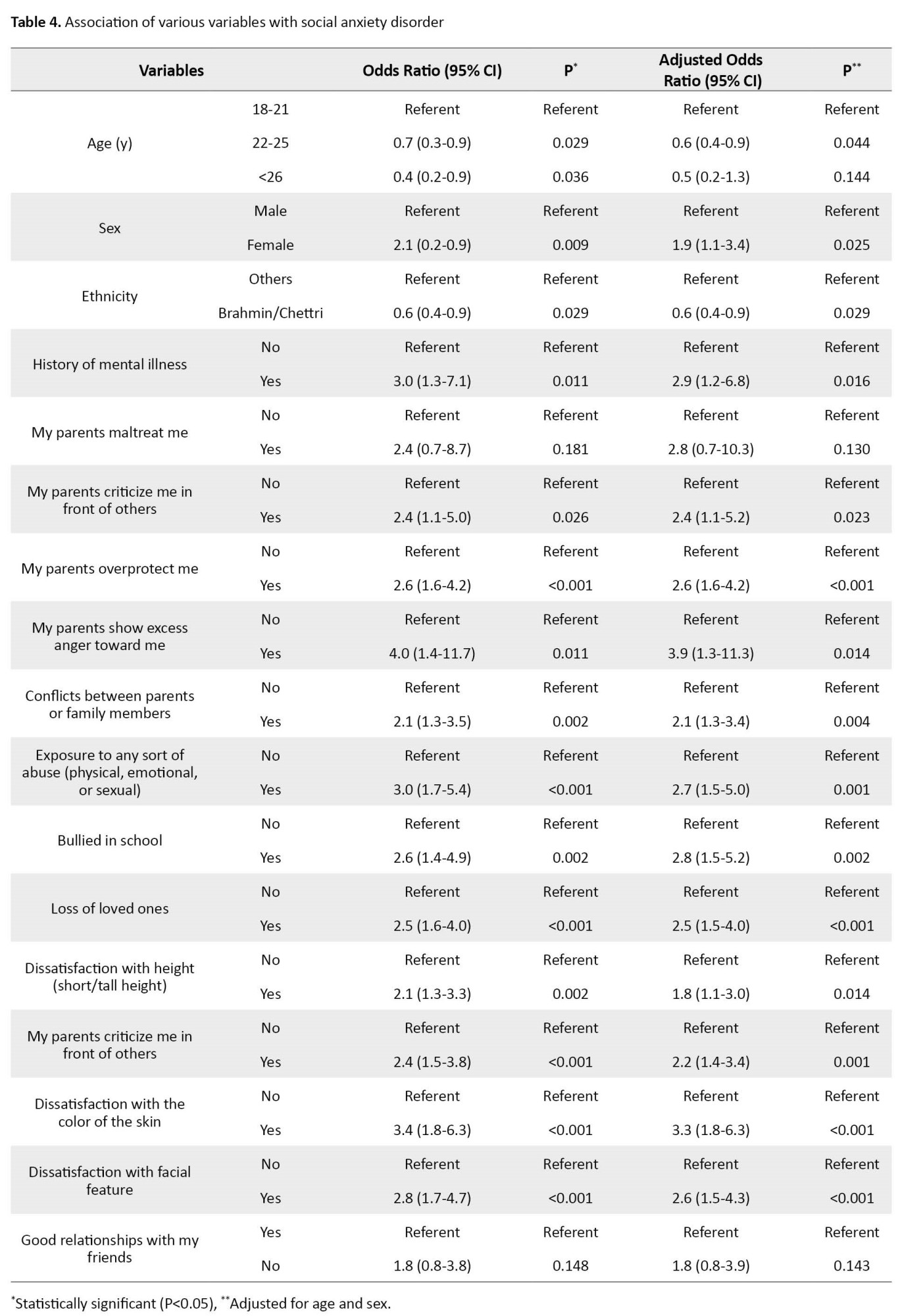
The odds of SAD were significantly higher among female participants (AOR=1.9; 95% CI, 1.1, 3.4), participants with a history of mental illness (AOR=2.9; 95% CI, 1.2, 6.8), those whose parents criticize them in front of others (AOR=2.4; 95% CI, 1.1, 5.2), parents who overprotect them (AOR=2.6; 95% CI, 1.6, 4.2), parents who show excess anger (AOR=3.9; 95% CI, 1.3, 11.3), participants experiencing conflicts with parents or family members (AOR=2.1; 95% CI, 1.3, 3.4), those exposed to any sort of abuse (AOR=2.7; 95% CI, 1.5, 5.0), participants who were bullied in school (AOR=2.8; 95% CI, 1.5, 5.2), those who experienced the loss of loved ones (AOR=2.5; 95% CI, 1.5, 4.0), participants dissatisfied with their height (AOR=1.8; 95% CI, 1.1, 3.0), those dissatisfied with their weight (AOR=2.2; 95% CI, 1.4, 3.4), participants dissatisfied with the color of their skin (AOR=3.3; 95% CI, 1.8, 6.3), and those participants dissatisfied with their facial features (AOR=2.6; 95% CI, 1.5, 4.3). Similarly, the Brahmin/Chettri ethnic group had lower odds of social anxiety disorders than other ethnic groups (AOR=0.6; 95% CI, 0.4, 0.9). In comparison to the age group of 18-21 years, the odds of SAD were lower among the age group 22-25 years (AOR=0.6; 95% CI, 0.4, 0.9) (Table 4).
Discussion
Among the 325 participants, 39.1% exhibited symptoms of SAD, which closely aligns with previous studies. For instance, a study conducted across seven countries reported a prevalence of 36% [12], while in Northwest Ethiopia, 40.2% of high school adolescents reported SAD [6]. Another study conducted in urban areas of Sonitpur district, Assam in India, found a prevalence of 38.3% [17]. Conversely, a study carried out in Khartoum State, Sudan, reported that 61.3% of medical students had SAD [1], and at the College of Education at the University of Garmian, more than 80% of students were affected [18]. We observed that mild SAD was the most common among participants (20.0%), followed by moderate, severe, and very severe, which is consistent with previously published literature [15, 19]. Furthermore, we found that 7.7% of participants had a history of mental illness, which closely aligns with a previous study [6].
Our findings indicate that the odds of SAD were significantly higher among female participants, as reported in previous studies [6, 20]. However, a study conducted among adolescents attending secondary schools in Enugu South East Nigeria reported that females were about twice as likely not to have anxiety compared to males [21]. This discrepancy may be attributed to differences in study tools, sample size, and geographical area.
Additionally, we found that the odds of SAD were higher among participants with a history of mental illness, similar to a previous study that reported higher odds among those with chronic illness and a family history of illness [6]. Moreover, we identified a significant association between social anxiety disorder and overprotective parents, consistent with studies indicating a positive correlation between child ratings of overprotection and social anxiety [22, 23]. Negative parenting styles, such as criticizing children in front of others, displaying excessive anger, and family conflicts were also significant risk factors for the development of SAD, which aligns with previous research [24].
Furthermore, we found a significant association between dissatisfaction with height and weight and SAD. This participants to previous studies that observed a strong link between body image anxiety and social phobia [25]. Similarly, we found significantly higher odds of SAD among participants dissatisfied with their facial features, consistent with a previous study [13]. Moreover, our study revealed that exposure to any form of abuse, such as physical, emotional, or sexual abuse, was a significant risk factor for SAD. While a previous study reported similar results, it specifically emphasized the stronger association between emotional factors and SAD [26, 27]. Lastly, participants who experienced bullying at school had higher odds of SAD, which aligns with previously published literature [28]. Furthermore, our study did not identify any association between religion, types of family, living arrangement, grade, parents’ education status, and occupation, which is similar to the findings reported in a previous study [6, 29].
Conclusion
This study revealed a high prevalence of SAD among the students. We also identified several significant risk factors associated with these disorders, including being female, having a history of mental illness, experiencing negative life events, such as conflicts between parents or family members, exposure to abuse, being bullied in school, and experiencing the loss of loved ones. Additionally, perceived parental behavior and individual appearance dissatisfaction were found to be contributing factors. Parents and college authorities must consider these factors to prevent and control SAD among students. We recommend further research and frequent studies on similar topics to deepen our understanding of this issue.
Study limitations
This cross-sectional study exclusively focused on health science students from selected colleges in Kathmandu City, Nepal. While employing a purposive sampling strategy, targeting health science students from five colleges in Kathmandu City, Nepal, the limited number of institutions included may restrict the generalizability of our findings to the broader student population in the city. Moreover, the utilization of a web-based survey format may have introduced social desirability bias, potentially leading participants to underreport social anxiety symptoms to present themselves more favorably.
To address these limitations, future research could benefit from expanding the sample size to include a more diverse range of colleges in Kathmandu City, Nepal or even extending the study to other geographic regions. Moreover, incorporating complementary methodologies, such as clinical interviews alongside self-report surveys could help mitigate the impact of social desirability bias and provide a more comprehensive understanding of social anxiety among health care students.
Ethical Considerations
Compliance with ethical guidelines
Before data collection, we obtained permission from the respective colleges, and ethical approval (Reference No.: 2079-92) was granted by the Institutional Review Committee of Yeti Health Science Academy. Written consent was obtained from the participating students, ensuring their voluntary participation without any financial incentives or coercion.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization: Rajesh Karki and Aarati Timsina; Methodology: Rajesh Karki and Aarati Timsina; Data curation: Aarati Timsina and Maheshor Kaphle; Formal analysis: Rajesh Karki and Ramswarth Sah; Writing the original draft: Rajesh Karki; Review and editing: Aarati Timsina, Maheshor Kaphle, and Ramswarth Sah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The sincerely thank the colleges for their cooperation and the participants for their valuable time and data. Their contributions were essential to this research.
References
Social anxiety disorder (SAD), also known as social phobia, is an anxiety disorder characterized by intense discomfort and anxiety related to potential rejection, humiliation, or negative evaluation in social situations [1]. Individuals afflicted by SAD may exhibit non-specific fears in ambiguous situations or specific tasks, such as public speaking or eating in the presence of others [2]. Initially recognized as a significant issue in the 19th century, the prevalence of social anxiety has surged over the 20th and 21st centuries, often referred to as the age of anxiety [3].
According to the World Health Organization (WHO), nearly 301 million individuals, including 58 million children and adolescents, were affected by anxiety disorders globally in 2019 [4]. Research findings suggest that the lifetime prevalence of SAD falls within the range of 3%–13%. Among university students globally, rates fluctuate from 9% to 16.1%, with notably higher rates observed in Ethiopia (26%) and India (31.1%) [5]. Moreover, data from studies across seven countries indicate that the lifetime prevalence of social phobia ranges from 22.9% to 57.6% [6].
SAD often coexists with other mental health conditions, such as eating disorders (comorbidity rates up to 60%) and mood disorders like depression and bipolar disorder (comorbidity rates ranging from 35% to 70% and 3.5% to 21%, respectively [7].
In Nepal, the mental health of adolescents is a major concern, with three-quarters of teenagers reporting anxiety in a nationwide study [8]. A study in the Dang District of Nepal found that nearly half of high school adolescents in grades 9 to 12 were affected by anxiety disorders [9]. Similarly, a study among undergraduate students of management in Kathmandu City, Nepal, revealed a higher prevalence of anxiety compared to stress and depression [10].
University students, who heavily rely on virtual social networks for communication, may be at increased risk for social anxiety due to the potential avoidance of face-to-face interaction [11].
Social anxiety, which disproportionately affects young people, is a rapidly growing phenomenon [12]. In today’s competitive environment, particularly among students, where high academic performance is emphasized, social anxiety disorder has become increasingly significant [13]. However, despite its prevalence, social anxiety disorder often remains underdiagnosed and undertreated [14]. Given the importance of social anxiety as an indicator of adult functioning, there is a dearth of studies evaluating its prevalence and impact specifically among Nepalese teenagers [8]. Therefore, this study investigates the prevalence of social anxiety disorders and identifies associated factors among bachelor-level health science students in Kathmandu City, Nepal.
Materials and Methods
Study design, area, and population
A web-based cross-sectional study was conducted in 2023 among health science students enrolled in bachelor-level programs, specifically bachelor’s degrees in public health, nursing, and post-basis bachelor of nursing, from five selected colleges in Kathmandu City, Nepal.
Sample size determination and sampling technique
The sample size for the study was determined using the formula n=Z2pq/d2, with an assumed prevalence of social phobia symptoms among students (p)=31.2% [15], a Z score of 1.96 for a 95% confidence level, and a desired margin of error (d) of 0.05. This calculation yielded a final sample size of 330. Given the occurrence of student vacations during the data collection period and potential imitations on response rates, we employed the purposive sampling technique. Specifically, we e-mailed all students enrolled in the respective programs at the five selected colleges in Kathmandu City, Nepal.
Data collection
A self-constructed structured questionnaire was used to measure the study objectives and distributed to participants. This questionnaire included three sections. The first section collected sociodemographic information, including age, sex, and relevant background characteristics. The second section explored factors potentially associated with SAD, such as perceived parental behavior, experience of negative life events, perceived individual appearance, and peer relationships. These questions were formulated after an extensive literature review. The third section addressed SAD measurement directly. A validated tool called the social phobia inventory (SPIN) was employed. This self-report questionnaire utilizes a 5-point Likert scale (ranging from “not at all” to “extremely”) for each of its 17 items. The total score on the SPIN ranges from 0 to 68, with higher scores indicating a greater degree of social anxiety [16].
Before data collection, the researchers obtained a list of students and their e-mail addresses from the respective colleges with appropriate permissions. The questionnaire was then e-mailed to all students, accompanied by clear instructions for completion. This approach aimed to maximize the potential participant pool while acknowledging the impact of the vacation period on response rates. The data collection period spanned from March 31st, 2023, to May 14th, 2023. However, due to the strict time frame of our study and the cessation of responses after this date, a total of 325 students actively participated, resulting in a response rate of 98.48%. This comprehensive e-mail distribution to all eligible students ensured that our response rate was maximized given the constraints of the study.
Prevalence of social anxiety disorder
To determine the prevalence of SAD among the participants, we utilized a cut-off score of 19 on SPIN. A score of 19 or higher indicates the presence of social phobia [17]. According to studies, the tool accurately predicts social anxiety in 78% of cases based on this cut-off score [16].
Validation of the questionnaire
The subject expert validated the questionnaire. To assess its reliability, we conducted a pre-testing on 10% of the total sample size within a similar area. The reliability was determined using the Cronbach α method, which yielded a calculated value of 0.95.
Data quality control
All responses were carefully reviewed daily to ensure consistency. The final set of responses was imported into the SPSS software, version 26, for identifying and addressing missing values and outliers. In case of any missing values or outliers, the respective participants were contacted again. Each variable was appropriately coded. All researchers actively participated in this stage of the process.
Data analysis and presentation
The data analysis was conducted using the SPSS software. Descriptive analysis was performed to calculate frequencies, percentages, Mean±SD for the socio-demographic factors and variables related to SAD. To identify the significant predictors of social anxiety disorder, a binary logistic regression model was utilized with a 95% confidence interval. The adjusted odds ratio (AOR) or odds ratio (OR) was estimated to quantify the strength of association between the independent variables (socio-demographic factors, perceived parental behavior, experience of negative life events, perceived individual appearance, peer relations) and the dependent variable (SAD). The statistical significance level was set at P<0.05. The findings included AOR/OR values, confidence intervals, and P for each predictor variable.
Results
Socio-demographic characteristics of the sample
Out of 325 participants, the study included a large portion of young adults aged 22-25 years (63.7%, n=207), with a mean age of 22.84±2.25 years. Females comprised most of the participants (74.8%, n=243). Regarding religion, Hinduism was the most prevalent faith (94.5%, n=307). Brahmin/Chettri emerged as the dominant caste (64.0%, n=208), and nuclear families were the most common family structure (74.8%, n=243). Nearly half (45.8%, n=149) of the participants resided with their parents, while only a small percentage (7.7%, n=25) reported a prior history of mental illness (Table 1).
Perceived parental behavior, experience of negative life events, perceived individual appearance, and peer relations
Perceived parental behavior
Only 3.1% (n=10) of the participants reported experiencing maltreatment from their parents, while 9.5% (n=31) mentioned that their parents criticized them in front of others. Furthermore, 32% (n=106) of the participants reported that their parents overprotect them, and a small percentage (5.2%, n=17) mentioned experiencing excess anger from their parents.
Experience of negative life events
Approximately 28.9% (n=94) of the participants reported conflicts between their parents or family members, while 18.2% (n=59) mentioned exposure to any sort of abuse. A notable percentage of participants (15.1%) reported being bullied in school, and the loss of loved ones was reported by 35.1% (n=114) of the participants.
Perceived individual appearance
Among the participants, 34.8% (n=113) mentioned dissatisfaction with their height (short/tall height), while 43.7% (n=142) expressed dissatisfaction with their weight (low/excess weight). A small percentage of participants (15.4%, n=50) reported dissatisfaction with the color of their skin, and 25.5% (n=83) mentioned dissatisfaction with their facial features.
Peer relations
The majority of participants (91.1%, n=296) mentioned having a good relationship with their friends, while only a small percentage (8.9%) reported having a poor relationship with their friends (Table 2).
Prevalence and level of social anxiety disorder
Out of the 325 participants, social anxiety disorder was present among 39.1% (n=127), with a mean score of 16.73±11.85. Categorically, the majority had mild social anxiety disorder (20.0%, n=65), while only 2.8% had severe, and 1.2% had a very severe level of SAD (Table 3).
Logistic regression analysis of factors associated with social anxiety disorder
A logistic regression analysis was performed to assess the association between selected variables and social anxiety disorder. Only variables that showed a significant association with social anxiety disorder were included in the model. The results revealed that the model was statistically significant, as indicated by the Omnibus tests of model coefficients (χ2=62.649, P<0.001). The model showed a good fit to the data, as indicated by the Hosmer and Lemeshow test (χ2=9.354, P=0.313), and a 0.2 Nagelkerke pseudo-R2 (Table 4).
The odds of SAD were significantly higher among female participants (AOR=1.9; 95% CI, 1.1, 3.4), participants with a history of mental illness (AOR=2.9; 95% CI, 1.2, 6.8), those whose parents criticize them in front of others (AOR=2.4; 95% CI, 1.1, 5.2), parents who overprotect them (AOR=2.6; 95% CI, 1.6, 4.2), parents who show excess anger (AOR=3.9; 95% CI, 1.3, 11.3), participants experiencing conflicts with parents or family members (AOR=2.1; 95% CI, 1.3, 3.4), those exposed to any sort of abuse (AOR=2.7; 95% CI, 1.5, 5.0), participants who were bullied in school (AOR=2.8; 95% CI, 1.5, 5.2), those who experienced the loss of loved ones (AOR=2.5; 95% CI, 1.5, 4.0), participants dissatisfied with their height (AOR=1.8; 95% CI, 1.1, 3.0), those dissatisfied with their weight (AOR=2.2; 95% CI, 1.4, 3.4), participants dissatisfied with the color of their skin (AOR=3.3; 95% CI, 1.8, 6.3), and those participants dissatisfied with their facial features (AOR=2.6; 95% CI, 1.5, 4.3). Similarly, the Brahmin/Chettri ethnic group had lower odds of social anxiety disorders than other ethnic groups (AOR=0.6; 95% CI, 0.4, 0.9). In comparison to the age group of 18-21 years, the odds of SAD were lower among the age group 22-25 years (AOR=0.6; 95% CI, 0.4, 0.9) (Table 4).
Discussion
Among the 325 participants, 39.1% exhibited symptoms of SAD, which closely aligns with previous studies. For instance, a study conducted across seven countries reported a prevalence of 36% [12], while in Northwest Ethiopia, 40.2% of high school adolescents reported SAD [6]. Another study conducted in urban areas of Sonitpur district, Assam in India, found a prevalence of 38.3% [17]. Conversely, a study carried out in Khartoum State, Sudan, reported that 61.3% of medical students had SAD [1], and at the College of Education at the University of Garmian, more than 80% of students were affected [18]. We observed that mild SAD was the most common among participants (20.0%), followed by moderate, severe, and very severe, which is consistent with previously published literature [15, 19]. Furthermore, we found that 7.7% of participants had a history of mental illness, which closely aligns with a previous study [6].
Our findings indicate that the odds of SAD were significantly higher among female participants, as reported in previous studies [6, 20]. However, a study conducted among adolescents attending secondary schools in Enugu South East Nigeria reported that females were about twice as likely not to have anxiety compared to males [21]. This discrepancy may be attributed to differences in study tools, sample size, and geographical area.
Additionally, we found that the odds of SAD were higher among participants with a history of mental illness, similar to a previous study that reported higher odds among those with chronic illness and a family history of illness [6]. Moreover, we identified a significant association between social anxiety disorder and overprotective parents, consistent with studies indicating a positive correlation between child ratings of overprotection and social anxiety [22, 23]. Negative parenting styles, such as criticizing children in front of others, displaying excessive anger, and family conflicts were also significant risk factors for the development of SAD, which aligns with previous research [24].
Furthermore, we found a significant association between dissatisfaction with height and weight and SAD. This participants to previous studies that observed a strong link between body image anxiety and social phobia [25]. Similarly, we found significantly higher odds of SAD among participants dissatisfied with their facial features, consistent with a previous study [13]. Moreover, our study revealed that exposure to any form of abuse, such as physical, emotional, or sexual abuse, was a significant risk factor for SAD. While a previous study reported similar results, it specifically emphasized the stronger association between emotional factors and SAD [26, 27]. Lastly, participants who experienced bullying at school had higher odds of SAD, which aligns with previously published literature [28]. Furthermore, our study did not identify any association between religion, types of family, living arrangement, grade, parents’ education status, and occupation, which is similar to the findings reported in a previous study [6, 29].
Conclusion
This study revealed a high prevalence of SAD among the students. We also identified several significant risk factors associated with these disorders, including being female, having a history of mental illness, experiencing negative life events, such as conflicts between parents or family members, exposure to abuse, being bullied in school, and experiencing the loss of loved ones. Additionally, perceived parental behavior and individual appearance dissatisfaction were found to be contributing factors. Parents and college authorities must consider these factors to prevent and control SAD among students. We recommend further research and frequent studies on similar topics to deepen our understanding of this issue.
Study limitations
This cross-sectional study exclusively focused on health science students from selected colleges in Kathmandu City, Nepal. While employing a purposive sampling strategy, targeting health science students from five colleges in Kathmandu City, Nepal, the limited number of institutions included may restrict the generalizability of our findings to the broader student population in the city. Moreover, the utilization of a web-based survey format may have introduced social desirability bias, potentially leading participants to underreport social anxiety symptoms to present themselves more favorably.
To address these limitations, future research could benefit from expanding the sample size to include a more diverse range of colleges in Kathmandu City, Nepal or even extending the study to other geographic regions. Moreover, incorporating complementary methodologies, such as clinical interviews alongside self-report surveys could help mitigate the impact of social desirability bias and provide a more comprehensive understanding of social anxiety among health care students.
Ethical Considerations
Compliance with ethical guidelines
Before data collection, we obtained permission from the respective colleges, and ethical approval (Reference No.: 2079-92) was granted by the Institutional Review Committee of Yeti Health Science Academy. Written consent was obtained from the participating students, ensuring their voluntary participation without any financial incentives or coercion.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization: Rajesh Karki and Aarati Timsina; Methodology: Rajesh Karki and Aarati Timsina; Data curation: Aarati Timsina and Maheshor Kaphle; Formal analysis: Rajesh Karki and Ramswarth Sah; Writing the original draft: Rajesh Karki; Review and editing: Aarati Timsina, Maheshor Kaphle, and Ramswarth Sah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The sincerely thank the colleges for their cooperation and the participants for their valuable time and data. Their contributions were essential to this research.
References
- Suleiman HA, Elamin SA, Alobeid AA, Altaib WE. Prevalence of social anxiety disorder among medical students from six medical schools in Khartoum State. Sudan Journal of Medical Sciences. 2021; 16(2):223-32. [DOI:10.18502/sjms.v16i2.9290]
- Melkam M, Segon T, Nakie G. Social phobia of Ethiopian students: Meta-analysis and systematic review. Systematic Reviews. 2023; 12(1):41. [DOI:10.1186/s13643-023-02208-2] [PMID]
- Murad OS. Social anxiety in relation to self-esteem among university students in Jordan. International Education Studies. 2020; 13(2):96-103. [DOI:10.5539/ies.v13n2p96]
- World Health Organization. Mental disorders. Geneva: World Health Organizatio; 2022. [Link]
- Al-Johani WM, AlShamlan NA, AlAmer NA, Shawkhan RA, Almayyad AH, Alghamdi LM, et al. Social anxiety disorder and its associated factors: A cross-sectional study among medical students, Saudi Arabia. BMC Psychiatry. 2022; 22(1):505. [DOI:10.1186/s12888-022-04147-z] [PMID]
- Nakie G, Melkam M, Desalegn GT, Zeleke TA. Prevalence and associated factors of social phobia among high school adolescents in Northwest Ethiopia, 2021. Frontiers in Psychiatry. 2022; 13:949124. [DOI:10.3389/fpsyt.2022.949124] [PMID]
- Koyuncu A, İnce E, Ertekin E, Tükel R. Comorbidity in social anxiety disorder: Diagnostic and therapeutic challenges. Drugs in Context. 2019; 8:212573. [DOI:10.7573/dic.212573] [PMID]
- Singh R, Singh B, Mahato S, Hambour VK. Social support, emotion regulation and mindfulness: A linkage towards social anxiety among adolescents attending secondary schools in Birgunj, Nepal. Plos One. 2020; 15(4):e0230991. [DOI:10.1371/journal.pone.0230991] [PMID]
- Bhandari K, Adhikari C. Prevalence and factors associated with anxiety disorder among secondary school adolescents of Dang district, Nepal. Journal of Gandaki Medical College. 2015; 8(1):64-7. [Link]
- Sharma K, Shakya A. Prevalence and factors associated with depression, anxiety, and stress among undergraduate management students in Kathmandu, Nepal. Journal of Community Medicine and Public Health Report. 2022; 3(6):1-9. [Link]
- Torkian S, Mohammadi NM, Mohammadizadeh M, Shahesmaeili A. Virtual social networks addiction and high-risk group among health science students in Iran: A latent class analysis. Iranian Journal of Health Sciences. 2022; 10(1). [DOI:10.18502/jhs.v10i1.9105]
- Jefferies P, Ungar M. Social anxiety in young people: A prevalence study in seven countries. Plos One. 2020; 15(9):e0239133. [DOI:10.1371/journal.pone.0239133] [PMID]
- Preeti PD. Prevalence of social anxiety disorder and its determinants among undergraduate medical students of East Delhi. International Journal of Community Medicine and Public Health. 2019; 6(3):1335-9. [DOI:10.18203/2394-6040.ijcmph20190636]
- Hakami RM, Mahfouz MS, Adawi AM, Mahha AJ, Athathi AJ, Daghreeri HH, et al. Social anxiety disorder and its impact in undergraduate students at Jazan University, Saudi Arabia. Mental Illness. 2017; 9(2):42-7. [DOI:10.1108/mi.2017.7274]
- Desalegn GT, Getinet W, Tadie G. The prevalence and correlates of social phobia among undergraduate health science students in Gondar, Gondar Ethiopia. BMC Research Notes. 2019; 12(1):438.[DOI:10.1186/s13104-019-4482-y] [PMID]
- Chukwujekwu D, Olose E. Validation of the social phobia inventory (Spin) in Nigeria. Journal of Psychiatry and Psychiatric Disorders. 2018; 2(2):49-54. [Link]
- Harikrishnan U, Ali A, Sobhana H. Prevalence of social phobia among school going adolescents. The International Journal of Indian Psychology. 2016; 4(74):181-4. [DOI:10.25215/0401.039]
- Ahmad RJ, Bayan H, Faque T, Seidi PA. Prevalence of social anxiety in students of college of education-university of Garmian. Journal of Arts, Science & Commerce. 2017; 3(1):79-83. [Link]
- Momeni M, Zeyghami R, Moradi M, Taherpour M, Sarichloo M. [Prevalence and factors associated with social phobia in nursing and midwifery students (Persian)]. Journal of Health and Care. 2015; 17(2):137-45. [Link]
- Karki A, Thapa B, Pradhan PMS, Basel P. Depression, anxiety and stress among high school students: A cross-sectional study in an urban municipality of Kathmandu, Nepal. PLoS Global Public Health. 2022; 2(5):e0000516. [DOI:10.1371/journal.pgph.0000516] [PMID]
- Chinawa AT, Onukwuli VO, Chinawa JM, Mayike PC, Nduagubam OC, Odinka PC, et al. Anxiety disorders among adolescents attending secondary schools in Enugu South East Nigeria. Current Pediatric Research. 2018; 22(3):239-48. [Link]
- Festa CC, Ginsburg GS. Parental and peer predictors of social anxiety in youth. Child Psychiatry & Human Development. 2011; 42:291-306. [DOI:10.1007/s10578-011-0215-8] [PMID]
- Knappe S, Beesdo-Baum K, Fehm L, Lieb R, Wittchen HU. Characterizing the association between parenting and adolescent social phobia. Journal of Anxiety Disorders. 2012; 26(5):608-16. [DOI:10.1016/j.janxdis.2012.02.014] [PMID]
- Olson CM. Familial factors in the development of social anxiety disorder. Journal of Psychosocial Nursing and Mental Health Services. 2021; 59(7):23-34. [DOI:10.3928/02793695-20210219-01] [PMID]
- Waghachavare VB, Quraishi SR, Dhumale GB, Gore AD. A cross-sectional study of correlation of body image anxiety with social phobia and their association with depression in the adolescents from a rural area of Sangli District in India. International Journal of Preventive Medicine. 2014; 5(12):1626-9. [PMID]
- Iffland B, Sansen LM, Catani C, Neuner F. Emotional but not physical maltreatment is independently related to psychopathology in subjects with various degrees of social anxiety: A web-based internet survey. BMC Psychiatry. 2012; 12:49. [DOI:10.1186/1471-244X-12-49] [PMID]
- Liu J, Deng J, Zhang H, Tang X. The relationship between child maltreatment and social anxiety: A meta-analysis. Journal of Affective Disorders. 2023; 329:157-67. [DOI:10.1016/j.jad.2023.02.081] [PMID]
- Pontillo M, Tata MC, Averna R, Demaria F, Gargiullo P, Guerrera S, et al. Peer victimization and onset of social anxiety disorder in children and adolescents. Brain Sciences. 2019; 9(6):132. [DOI:10.3390/brainsci9060132] [PMID]
- Pokharel S, Chapagain S, Shrestha S. Anxiety among secondary school adolescents of Bharatpur Metropolitan City, Chitwan. Journal of Chitwan Medical College. 2022; 12(2):30-34. [DOI:10.54530/jcmc.724]
Type of Study: Original Article |
Subject:
Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
