

Volume 13, Issue 2 (Spring 2025)
Iran J Health Sci 2025, 13(2): 115-122 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abayabay I D, Al Ali C A C, Alava K M, Aquino T A J, Autor Y B J, Baltazar R J R, et al . Menstrual Health Literacy Among Young Female Adults in Northern Mindanao: A Descriptive Cross-sectional Study. Iran J Health Sci 2025; 13 (2) :115-122
URL: http://jhs.mazums.ac.ir/article-1-1003-en.html
URL: http://jhs.mazums.ac.ir/article-1-1003-en.html
Izzy D. Abayabay 

 , Chariefa Aaliyah C. Al Ali , Kyramae M. Alava , Trisha Andree J. Aquino , Yuri Benedict J. Autor , Ranieza Jazz R. Baltazar , Jasmine Kyle C. Casicas , Ma. Melevir Madelyn A. Castañares , Cristine M. Dulfo , Raenah Patrizia B. Dy , Paolo B. Araune * , Rodesa Shaira B. Cornito
, Chariefa Aaliyah C. Al Ali , Kyramae M. Alava , Trisha Andree J. Aquino , Yuri Benedict J. Autor , Ranieza Jazz R. Baltazar , Jasmine Kyle C. Casicas , Ma. Melevir Madelyn A. Castañares , Cristine M. Dulfo , Raenah Patrizia B. Dy , Paolo B. Araune * , Rodesa Shaira B. Cornito
, Chariefa Aaliyah C. Al Ali , Kyramae M. Alava , Trisha Andree J. Aquino , Yuri Benedict J. Autor , Ranieza Jazz R. Baltazar , Jasmine Kyle C. Casicas , Ma. Melevir Madelyn A. Castañares , Cristine M. Dulfo , Raenah Patrizia B. Dy , Paolo B. Araune * , Rodesa Shaira B. Cornito
Department of Mathematics, College of Arts and Sciences, Xavier University-Ateneo de Cagayan, Cagayan de Oro, Philippines. , paraune@xu.edu.ph
Keywords: Menstrual health literacy (MHL), Young female adults, Education, Menstrual practices, Cultural influences
Full-Text [PDF 633 kb]
(52 Downloads)
| Abstract (HTML) (372 Views)
Full-Text: (1 Views)
Introduction
Menstruation, a fundamental biological process, continues to be shrouded in stigma, silence and cultural taboos in many parts of the world, often leading to poor menstrual health literacy (MHL) among young female adults [1]. This lack of awareness and understanding negatively impacts menstrual health management, with cultural and socioeconomic factors playing a crucial role in shaping perceptions and practices surrounding menstruation. However, a precise and unified definition of “MHL” remains elusive in the existing literature, contributing to inconsistencies in how the concept is understood and measured.
MHL refers to an individual’s ability to access, comprehend, and apply information about menstruation, menstrual hygiene, and reproductive health [1]. This issue includes understanding the menstrual cycle, the proper management of menstrual hygiene, and the sociocultural beliefs influencing these practices. While international studies have shown that educational attainment, cultural influences and socioeconomic factors are significantly associated with MHL, there is a gap in research explicitly focused on young female adults in Northern Mindanao, Philippines. This study aims to fill that gap by investigating how these factors contribute to MHL in this particular context.
Previous studies in other regions have revealed that inadequate menstrual health education can lead to misconceptions and poor menstrual hygiene management. For instance, in Afghanistan, young females had limited knowledge about menstruation due to a lack of proper education before menarche, with their primary source of information being their mothers [2]. Similarly, poor access to sanitary facilities in Nigerian schools hindered proper menstrual health management [3] and in Bangladesh, cultural restrictions and social stigma significantly shaped menstrual beliefs and practices [4].
While global efforts, such as integrating menstrual health management (MHM) programs in schools, have improved awareness and access to menstrual resources [5], there remains a significant gap in addressing the impact of cultural and socioeconomic barriers, especially in rural and less educated populations. Studies on the relationship between cultural beliefs, socioeconomic status, and MHL in the Philippines are scarce, with a few studies pointing to disparities in menstrual education and practices between urban and rural areas.
This study explores the level of MHL among young female adults in Northern Mindanao, Philippines, focusing on their awareness of menstrual hygiene, menstrual beliefs, practices and the types of menstrual materials used. It also examines the influence of geographical location and socioeconomic status on MHL to contribute to the growing research on MHL in Southeast Asia.
Materials and Methods
Research design
This study employed a descriptive cross-sectional design to assess MHL among young female adults. A descriptive design enabled the researchers to examine menstrual beliefs, practices and awareness simultaneously without manipulating variables. This approach provided a snapshot of the population’s characteristics, offering insights into how factors such as cultural influences, educational background, and socioeconomic status were associated with MHL.
Sample, sample size and sampling technique
This study utilized simple random sampling to select participants from urban and rural barangays in Northern Mindanao, targeting young female adults aged 18 to 25 years, as this age range represents a critical transition period where MHL significantly influences menstrual practices and overall well-being. The population sizes were 470 for urban and 842 for rural barangays. Using the Cochran formula, the required sample sizes were 212 for urban and 265 for rural areas, ensuring statistical reliability and generalizability [6]. Participants were included if they were biologically female, aged 18 to 25 and were permanent residents of the selected barangays. However, those with medical conditions affecting menstruation (e.g. polycystic ovary syndrome, amenorrhea), those who were pregnant or breastfeeding, and those who had received specialized menstrual health education beyond standard school curricula were excluded. Data collection was conducted on-site, with participants self-administering a researcher-developed questionnaire, designed based on validated MHL frameworks and pre-tested for reliability. Trained field researchers were available to provide clarifications when necessary, ensuring accurate responses while maintaining participant independence. This randomized selection approach ensured an unbiased and representative sample, allowing significant comparisons between urban and rural participants.
Data collection process
The data collection process involved review, approval, and revision stages. Initially, the paper underwent a series of revisions based on feedback from the research panelists. Following these revisions, the research instrument was validated by a research validator approved by the research mentor, incorporating further suggestions for improvement. A pilot test with 30 participants used the Cronbach α to test the instrument’s reliability. After confirming reliability, the research protocol, informed consent forms and the research instrument were submitted to the Research Ethics Committee (REC) for approval. Revisions recommended by the REC were made, and final approval was obtained. Data collection commenced with selecting respondents through simple random sampling from urban and rural barangays in Northern Mindanao. For permission, formal letters were sent to local officials and the research questionnaires were distributed to identified respondents. Informed consent was explained and obtained before participation. The questionnaire included 30 statements and four demographics, answered on a 4-point Likert scale. Collected data were securely stored, with hard copies in a locked cabinet and soft copies in a restricted Google Drive accessible only to the research team. Confidentiality and privacy of respondents were maintained throughout the study. Once the research paper was evaluated, revised and approved, it was made available to relevant stakeholders.
The instrument of data collection
The study utilized a structured 28-item close-ended questionnaire adapted from existing validated instruments, including the menstrual practices questionnaire [7], with modifications to incorporate culturally relevant questions specific to the Filipino context. The researchers designed the questionnaire with input from public health experts and MHL, ensuring alignment with established frameworks. It consisted of demographics, menstrual beliefs, and awareness of proper menstrual hygiene. The demographics section included four questions on educational attainment, geographical location, and menstrual materials used at home and away, taking approximately 2 minutes to complete. The menstrual beliefs section contained 10 Likert-scale questions assessing prevalent beliefs and cultural taboos surrounding menstruation in the Philippines, such as myths about bathing during menstruation, requiring about five minutes to complete. The awareness section was divided into two subsegments: The first one assessed knowledge of proper menstrual hygiene routines, and the second evaluated current menstrual practices, both using a Likert scale, with each subsegment containing 9 questions and requiring approximately 10 minutes to complete. Responses were scored on a 4-point Likert scale, with higher scores indicating greater awareness and adherence to proper menstrual health practices. The questionnaire underwent expert content validation to ensure relevance and clarity, and pilot testing was conducted among a small sample of young female adults not included in the final study to assess reliability. The Cronbach α was used to measure internal consistency, confirming the instrument’s reliability for assessing MHL within the target population.
Data analysis
The study employed inferential statistical methods to analyze the relationship between menstrual health awareness and various demographic factors among young female adults in Northern Mindanao. To compare differences in awareness based on educational attainment and the type of menstrual materials used, a one-way analysis of variance (ANOVA) test was conducted to assess significant variations between multiple categorical groups [8]. A t-test was used to determine significant mean differences in awareness levels between urban and rural respondents [9]. The Pearson correlation was also applied to examine the correlation between menstrual health awareness and menstrual beliefs, identifying potential positive or negative relationships [10].
Results
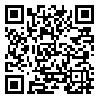
The study analyzed respondents’ awareness of proper menstrual hygiene based on their educational attainment. The sample included individuals with varying educational backgrounds, ranging from those who did not attend formal education to college graduates. Before statistical analyses, assumptions of normality and homogeneity of variances were tested using the Shapiro-Wilk and Levene’s tests, respectively. The normality assumption was met and the homogeneity of variances was confirmed, justifying the use of one-way ANOVA.
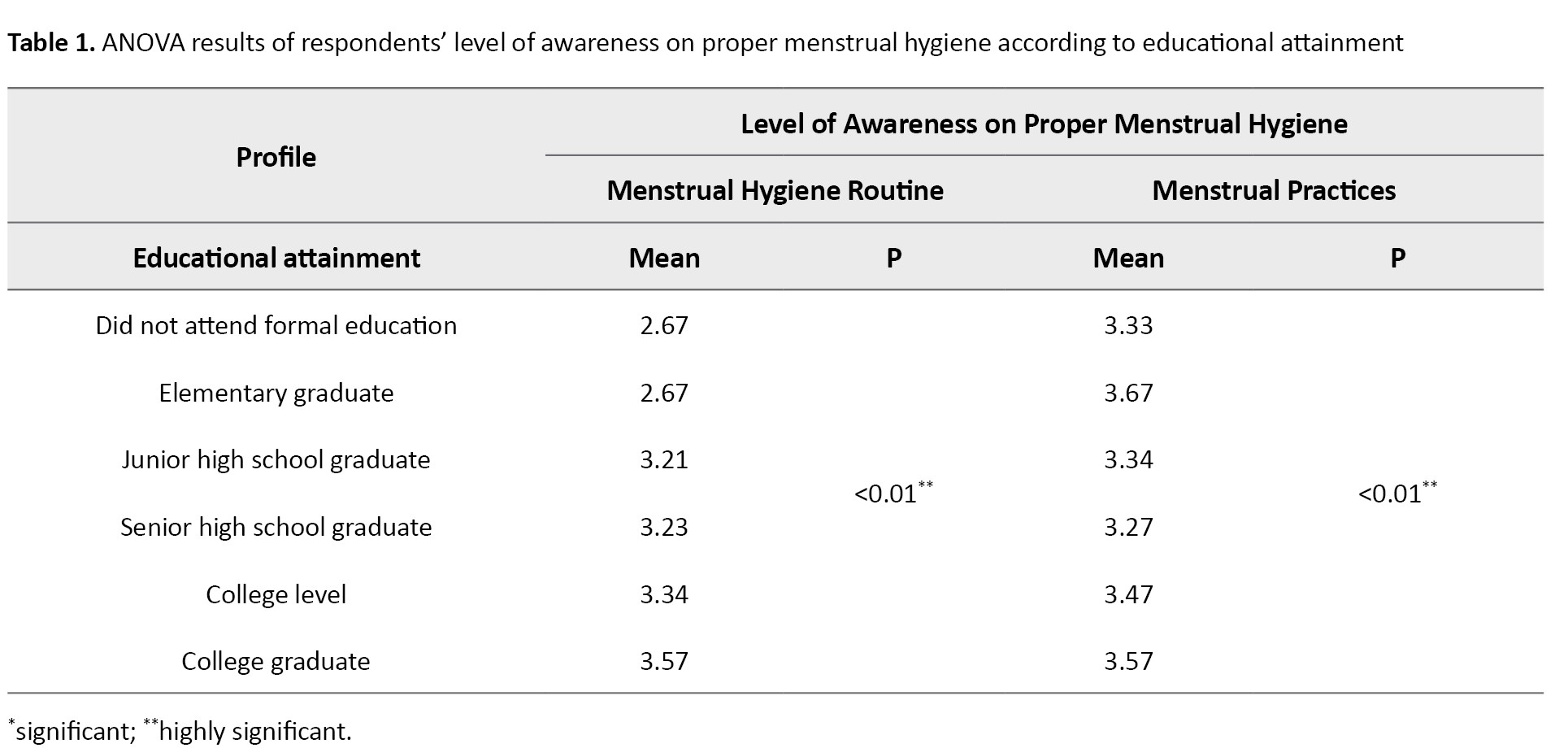
Table 1 presents the ANOVA results comparing awareness levels in two aspects: Menstrual hygiene routine and menstrual practices. The one-way ANOVA revealed highly significant differences in menstrual hygiene routine awareness across educational attainment levels (P<0.01). Post-hoc analysis using the Tukey HSD test indicated that respondents with a college degree had the highest mean awareness score (mean=3.57), significantly higher than those who did not attend formal education or completed only elementary education (mean=2.67, P<0.01). Similarly, for menstrual practices, ANOVA results showed significant differences (P<0.01), with college graduates having the highest awareness score (mean=3.57). Tukey HSD further confirmed that those without formal education had significantly lower scores (mean=3.33, P<0.01).
An independent t-test was conducted to determine whether respondents’ geographic location influenced menstrual hygiene awareness (Table 2).
The assumptions of normality and homogeneity of variances were tested and met. Results showed no significant difference in understanding of menstrual hygiene routines between respondents from urban and rural areas (P=0.561), suggesting that location does not impact routine awareness. However, for menstrual practices, a significant difference was found (P=0.026*), with rural respondents having a slightly higher mean awareness score (mean=3.45) compared to urban respondents (mean=3.37).
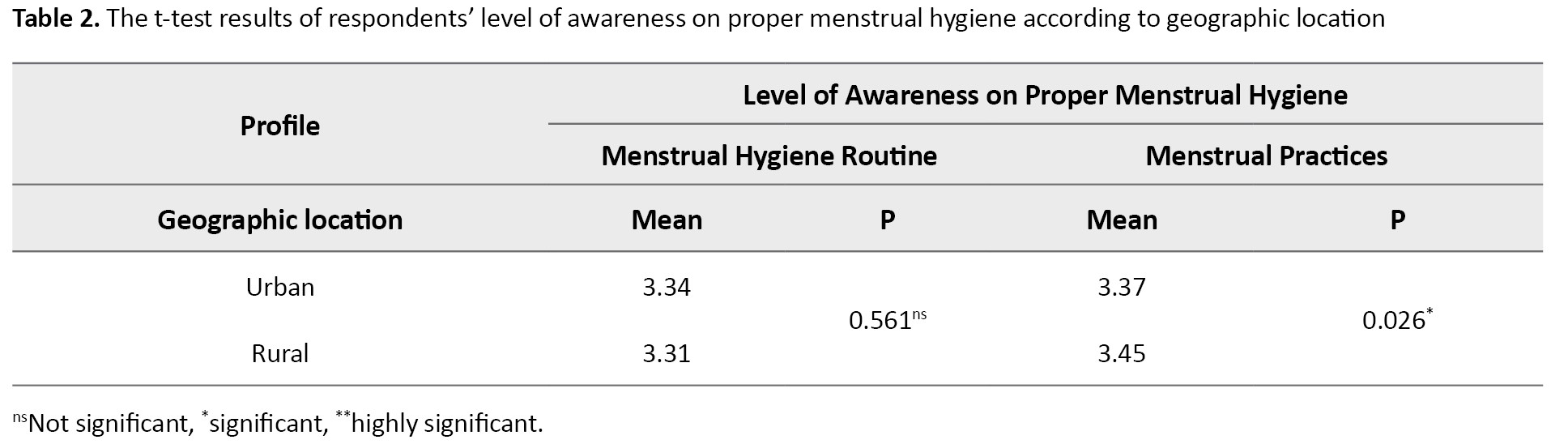
Table 3 presents the ANOVA results for awareness of menstrual hygiene by type of menstrual material used.
Assumptions of normality and homogeneity of variances were tested and met. A one-way ANOVA revealed highly significant differences in menstrual hygiene routine awareness across different menstrual materials (P<0.01**). Post hoc Tukey HSD analysis showed that respondents using tampons had the highest awareness score (mean=3.71), significantly higher than those using cloth/towels (mean=3.06, P<0.01). Similarly, for menstrual practices, significant differences were observed (P<0.01**), with respondents using reusable sanitary pads scoring the highest (mean=3.51), while those using cloth/towels had the lowest awareness score (mean=3.15).
Table 4 presents the Pearson correlation results assessing the relationship between awareness of proper menstrual hygiene and menstrual beliefs.
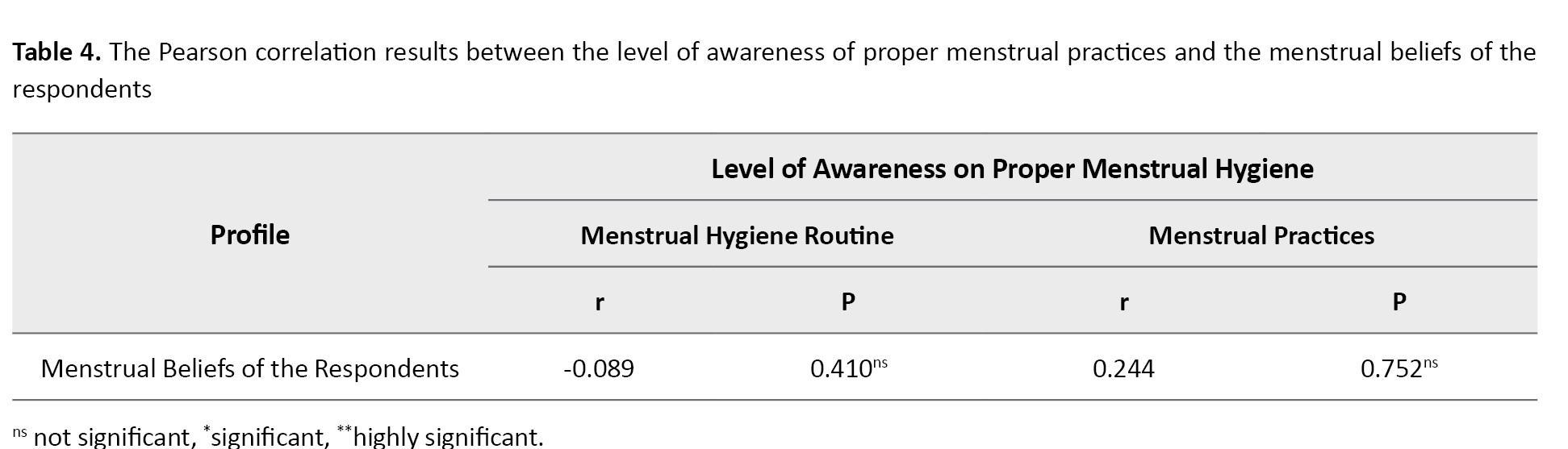
Assumptions of normality and linearity were tested and confirmed before conducting the analysis. Results showed a weak negative correlation (r=-0.089) between awareness of menstrual hygiene routines and menstrual beliefs. However, with a P=0.410, this correlation was not statistically significant, indicating that the observed relationship could be due to chance. Similarly, for menstrual practices, a weak positive correlation was found (r=0.244), but the P=0.752 suggested no significant relationship.
Discussion
The findings highlight the crucial role of educational attainment in shaping young female adults’ awareness of proper menstrual hygiene routines and practices. This finding aligns with Roy et al. who found that higher education levels significantly predict better menstrual hygiene practices, reinforcing the importance of education in fostering hygienic behaviors [11]. Similarly, Parasuraman et al. demonstrated that targeted health education interventions improved menstrual knowledge, attitudes, and practices, suggesting that formal education can enhance awareness beyond cultural or familial teachings [12].
Interestingly, the study found that individuals with elementary-level education demonstrated notable awareness of menstrual practices, a result that could be linked to traditional beliefs and practices passed down through generations. This finding contrasts with findings from other regions, where higher educational attainment generally correlates with increased awareness [13]. The discrepancy may be attributed to differences in the cultural transmission of menstrual knowledge, where informal yet consistent exposure to menstrual practices in rural communities complements formal education.
Geographic location also plays a role in menstrual awareness, with rural participants exhibiting slightly higher awareness of menstrual practices than their urban counterparts. This issue diverges from studies conducted in other settings, where urban respondents typically display higher awareness due to better access to health resources and education [14]. The present findings suggest that rural communities may rely more on traditional knowledge and local networks for menstrual health education, a trend also noted by Karjee et al., who emphasized the impact of community-based learning on menstrual health outcomes [13]. However, disparities in access to accurate menstrual information remain, underscoring the need for structured awareness programs to bridge knowledge gaps between urban and rural populations.
The study further reveals that menstrual material choices influence awareness levels, with respondents using tampons and reusable sanitary pads demonstrating higher awareness than those using cloth or towels. This finding is consistent with Shannon et al., who found that access to modern menstrual products promotes better hygiene and increases awareness of proper practices [15]. Conversely, respondents using cloths or towels exhibited lower awareness, aligning with Ritika et al. who attributed such practices to poverty and entrenched sociocultural norms [16]. These findings suggest that limited access to modern menstrual products, coupled with resistance to change, perpetuates lower awareness and outdated hygiene practices, highlighting the need for interventions that provide resources and challenge cultural misconceptions.
The weak positive correlation between awareness of proper menstrual hygiene and menstrual beliefs underscores the complex relationship between knowledge and traditional perceptions. Tshomo et al. noted that increased menstrual knowledge was associated with a reduced endorsement of menstrual taboos, as better-informed women were less likely to impose self-restrictions [17]. Similarly, Karout found that cultural beliefs influenced Saudi nursing students’ adherence to menstrual restrictions, illustrating how societal norms can override scientific understanding [18]. These findings suggest that while increased awareness is beneficial, deeper cultural shifts are required to dismantle menstrual taboos and encourage evidence-based practices.
Conclusion
The study concluded that educational attainment and the type of menstrual material used were significant factors in determining young female adults’ awareness of proper menstrual hygiene, with higher education levels and modern menstrual products correlating with increased awareness. Geographic location influenced awareness of menstrual practices but not hygiene routines, with rural areas showing slightly higher awareness levels. Despite these findings, there was no significant correlation between menstrual hygiene awareness and menstrual beliefs, highlighting the complexity of changing deep-seated cultural norms. These results underscore the need for targeted educational interventions and the promotion of modern menstrual products to enhance MHL and practices, ultimately improving menstrual health outcomes for young female adults.
Study limitations
Despite its significant findings, this study has several limitations. First, the study relied on self-reported data, which may be subject to response bias, as participants might have overestimated or underestimated their awareness of menstrual hygiene. Second, the study focused on a specific population, limiting the generalizability of the results to other regions or demographic groups with different cultural and socioeconomic backgrounds. Third, while the study examined the influence of education and geographic location, it did not account for other potential factors, such as access to menstrual hygiene products, exposure to health education programs, and family influence, which may have affected the respondents’ awareness levels. The study did not include a qualitative component, which could have provided deeper insights into the cultural and social factors influencing menstrual hygiene awareness. Future research should address these limitations by incorporating a more diverse sample, exploring additional influencing factors and utilizing mixed-method approaches to gain a more comprehensive understanding of menstrual health awareness.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of the Xavier Ateneo Research Ethics Board (Code: XU REC Package No. NSG-2024001285). Informed consent was obtained from all participants before their inclusion in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
conceptualization, data analysis and wrote the original draft: Izzy D. Abayabay, Chariefa Aaliyah C. Al Ali and Rodesa Shaira B. Cornito; Study design, data collection and revising the manuscript: Kyramae M. Alava, Yuri Benedict J. Autor, Ranieza Jazz R. Baltazar and Jasmine Kyle C. Casicas; Data interpretation and the literature review: Ma. Melevir Madelyn A. Castañares, Cristine M. Dulfo and Raenah Patrizia B. Dy; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all participants in this study for their time and cooperation.
References
Menstruation, a fundamental biological process, continues to be shrouded in stigma, silence and cultural taboos in many parts of the world, often leading to poor menstrual health literacy (MHL) among young female adults [1]. This lack of awareness and understanding negatively impacts menstrual health management, with cultural and socioeconomic factors playing a crucial role in shaping perceptions and practices surrounding menstruation. However, a precise and unified definition of “MHL” remains elusive in the existing literature, contributing to inconsistencies in how the concept is understood and measured.
MHL refers to an individual’s ability to access, comprehend, and apply information about menstruation, menstrual hygiene, and reproductive health [1]. This issue includes understanding the menstrual cycle, the proper management of menstrual hygiene, and the sociocultural beliefs influencing these practices. While international studies have shown that educational attainment, cultural influences and socioeconomic factors are significantly associated with MHL, there is a gap in research explicitly focused on young female adults in Northern Mindanao, Philippines. This study aims to fill that gap by investigating how these factors contribute to MHL in this particular context.
Previous studies in other regions have revealed that inadequate menstrual health education can lead to misconceptions and poor menstrual hygiene management. For instance, in Afghanistan, young females had limited knowledge about menstruation due to a lack of proper education before menarche, with their primary source of information being their mothers [2]. Similarly, poor access to sanitary facilities in Nigerian schools hindered proper menstrual health management [3] and in Bangladesh, cultural restrictions and social stigma significantly shaped menstrual beliefs and practices [4].
While global efforts, such as integrating menstrual health management (MHM) programs in schools, have improved awareness and access to menstrual resources [5], there remains a significant gap in addressing the impact of cultural and socioeconomic barriers, especially in rural and less educated populations. Studies on the relationship between cultural beliefs, socioeconomic status, and MHL in the Philippines are scarce, with a few studies pointing to disparities in menstrual education and practices between urban and rural areas.
This study explores the level of MHL among young female adults in Northern Mindanao, Philippines, focusing on their awareness of menstrual hygiene, menstrual beliefs, practices and the types of menstrual materials used. It also examines the influence of geographical location and socioeconomic status on MHL to contribute to the growing research on MHL in Southeast Asia.
Materials and Methods
Research design
This study employed a descriptive cross-sectional design to assess MHL among young female adults. A descriptive design enabled the researchers to examine menstrual beliefs, practices and awareness simultaneously without manipulating variables. This approach provided a snapshot of the population’s characteristics, offering insights into how factors such as cultural influences, educational background, and socioeconomic status were associated with MHL.
Sample, sample size and sampling technique
This study utilized simple random sampling to select participants from urban and rural barangays in Northern Mindanao, targeting young female adults aged 18 to 25 years, as this age range represents a critical transition period where MHL significantly influences menstrual practices and overall well-being. The population sizes were 470 for urban and 842 for rural barangays. Using the Cochran formula, the required sample sizes were 212 for urban and 265 for rural areas, ensuring statistical reliability and generalizability [6]. Participants were included if they were biologically female, aged 18 to 25 and were permanent residents of the selected barangays. However, those with medical conditions affecting menstruation (e.g. polycystic ovary syndrome, amenorrhea), those who were pregnant or breastfeeding, and those who had received specialized menstrual health education beyond standard school curricula were excluded. Data collection was conducted on-site, with participants self-administering a researcher-developed questionnaire, designed based on validated MHL frameworks and pre-tested for reliability. Trained field researchers were available to provide clarifications when necessary, ensuring accurate responses while maintaining participant independence. This randomized selection approach ensured an unbiased and representative sample, allowing significant comparisons between urban and rural participants.
Data collection process
The data collection process involved review, approval, and revision stages. Initially, the paper underwent a series of revisions based on feedback from the research panelists. Following these revisions, the research instrument was validated by a research validator approved by the research mentor, incorporating further suggestions for improvement. A pilot test with 30 participants used the Cronbach α to test the instrument’s reliability. After confirming reliability, the research protocol, informed consent forms and the research instrument were submitted to the Research Ethics Committee (REC) for approval. Revisions recommended by the REC were made, and final approval was obtained. Data collection commenced with selecting respondents through simple random sampling from urban and rural barangays in Northern Mindanao. For permission, formal letters were sent to local officials and the research questionnaires were distributed to identified respondents. Informed consent was explained and obtained before participation. The questionnaire included 30 statements and four demographics, answered on a 4-point Likert scale. Collected data were securely stored, with hard copies in a locked cabinet and soft copies in a restricted Google Drive accessible only to the research team. Confidentiality and privacy of respondents were maintained throughout the study. Once the research paper was evaluated, revised and approved, it was made available to relevant stakeholders.
The instrument of data collection
The study utilized a structured 28-item close-ended questionnaire adapted from existing validated instruments, including the menstrual practices questionnaire [7], with modifications to incorporate culturally relevant questions specific to the Filipino context. The researchers designed the questionnaire with input from public health experts and MHL, ensuring alignment with established frameworks. It consisted of demographics, menstrual beliefs, and awareness of proper menstrual hygiene. The demographics section included four questions on educational attainment, geographical location, and menstrual materials used at home and away, taking approximately 2 minutes to complete. The menstrual beliefs section contained 10 Likert-scale questions assessing prevalent beliefs and cultural taboos surrounding menstruation in the Philippines, such as myths about bathing during menstruation, requiring about five minutes to complete. The awareness section was divided into two subsegments: The first one assessed knowledge of proper menstrual hygiene routines, and the second evaluated current menstrual practices, both using a Likert scale, with each subsegment containing 9 questions and requiring approximately 10 minutes to complete. Responses were scored on a 4-point Likert scale, with higher scores indicating greater awareness and adherence to proper menstrual health practices. The questionnaire underwent expert content validation to ensure relevance and clarity, and pilot testing was conducted among a small sample of young female adults not included in the final study to assess reliability. The Cronbach α was used to measure internal consistency, confirming the instrument’s reliability for assessing MHL within the target population.
Data analysis
The study employed inferential statistical methods to analyze the relationship between menstrual health awareness and various demographic factors among young female adults in Northern Mindanao. To compare differences in awareness based on educational attainment and the type of menstrual materials used, a one-way analysis of variance (ANOVA) test was conducted to assess significant variations between multiple categorical groups [8]. A t-test was used to determine significant mean differences in awareness levels between urban and rural respondents [9]. The Pearson correlation was also applied to examine the correlation between menstrual health awareness and menstrual beliefs, identifying potential positive or negative relationships [10].
Results
The study analyzed respondents’ awareness of proper menstrual hygiene based on their educational attainment. The sample included individuals with varying educational backgrounds, ranging from those who did not attend formal education to college graduates. Before statistical analyses, assumptions of normality and homogeneity of variances were tested using the Shapiro-Wilk and Levene’s tests, respectively. The normality assumption was met and the homogeneity of variances was confirmed, justifying the use of one-way ANOVA.
Table 1 presents the ANOVA results comparing awareness levels in two aspects: Menstrual hygiene routine and menstrual practices. The one-way ANOVA revealed highly significant differences in menstrual hygiene routine awareness across educational attainment levels (P<0.01). Post-hoc analysis using the Tukey HSD test indicated that respondents with a college degree had the highest mean awareness score (mean=3.57), significantly higher than those who did not attend formal education or completed only elementary education (mean=2.67, P<0.01). Similarly, for menstrual practices, ANOVA results showed significant differences (P<0.01), with college graduates having the highest awareness score (mean=3.57). Tukey HSD further confirmed that those without formal education had significantly lower scores (mean=3.33, P<0.01).
An independent t-test was conducted to determine whether respondents’ geographic location influenced menstrual hygiene awareness (Table 2).
The assumptions of normality and homogeneity of variances were tested and met. Results showed no significant difference in understanding of menstrual hygiene routines between respondents from urban and rural areas (P=0.561), suggesting that location does not impact routine awareness. However, for menstrual practices, a significant difference was found (P=0.026*), with rural respondents having a slightly higher mean awareness score (mean=3.45) compared to urban respondents (mean=3.37).
Table 3 presents the ANOVA results for awareness of menstrual hygiene by type of menstrual material used.
Assumptions of normality and homogeneity of variances were tested and met. A one-way ANOVA revealed highly significant differences in menstrual hygiene routine awareness across different menstrual materials (P<0.01**). Post hoc Tukey HSD analysis showed that respondents using tampons had the highest awareness score (mean=3.71), significantly higher than those using cloth/towels (mean=3.06, P<0.01). Similarly, for menstrual practices, significant differences were observed (P<0.01**), with respondents using reusable sanitary pads scoring the highest (mean=3.51), while those using cloth/towels had the lowest awareness score (mean=3.15).
Table 4 presents the Pearson correlation results assessing the relationship between awareness of proper menstrual hygiene and menstrual beliefs.
Assumptions of normality and linearity were tested and confirmed before conducting the analysis. Results showed a weak negative correlation (r=-0.089) between awareness of menstrual hygiene routines and menstrual beliefs. However, with a P=0.410, this correlation was not statistically significant, indicating that the observed relationship could be due to chance. Similarly, for menstrual practices, a weak positive correlation was found (r=0.244), but the P=0.752 suggested no significant relationship.
Discussion
The findings highlight the crucial role of educational attainment in shaping young female adults’ awareness of proper menstrual hygiene routines and practices. This finding aligns with Roy et al. who found that higher education levels significantly predict better menstrual hygiene practices, reinforcing the importance of education in fostering hygienic behaviors [11]. Similarly, Parasuraman et al. demonstrated that targeted health education interventions improved menstrual knowledge, attitudes, and practices, suggesting that formal education can enhance awareness beyond cultural or familial teachings [12].
Interestingly, the study found that individuals with elementary-level education demonstrated notable awareness of menstrual practices, a result that could be linked to traditional beliefs and practices passed down through generations. This finding contrasts with findings from other regions, where higher educational attainment generally correlates with increased awareness [13]. The discrepancy may be attributed to differences in the cultural transmission of menstrual knowledge, where informal yet consistent exposure to menstrual practices in rural communities complements formal education.
Geographic location also plays a role in menstrual awareness, with rural participants exhibiting slightly higher awareness of menstrual practices than their urban counterparts. This issue diverges from studies conducted in other settings, where urban respondents typically display higher awareness due to better access to health resources and education [14]. The present findings suggest that rural communities may rely more on traditional knowledge and local networks for menstrual health education, a trend also noted by Karjee et al., who emphasized the impact of community-based learning on menstrual health outcomes [13]. However, disparities in access to accurate menstrual information remain, underscoring the need for structured awareness programs to bridge knowledge gaps between urban and rural populations.
The study further reveals that menstrual material choices influence awareness levels, with respondents using tampons and reusable sanitary pads demonstrating higher awareness than those using cloth or towels. This finding is consistent with Shannon et al., who found that access to modern menstrual products promotes better hygiene and increases awareness of proper practices [15]. Conversely, respondents using cloths or towels exhibited lower awareness, aligning with Ritika et al. who attributed such practices to poverty and entrenched sociocultural norms [16]. These findings suggest that limited access to modern menstrual products, coupled with resistance to change, perpetuates lower awareness and outdated hygiene practices, highlighting the need for interventions that provide resources and challenge cultural misconceptions.
The weak positive correlation between awareness of proper menstrual hygiene and menstrual beliefs underscores the complex relationship between knowledge and traditional perceptions. Tshomo et al. noted that increased menstrual knowledge was associated with a reduced endorsement of menstrual taboos, as better-informed women were less likely to impose self-restrictions [17]. Similarly, Karout found that cultural beliefs influenced Saudi nursing students’ adherence to menstrual restrictions, illustrating how societal norms can override scientific understanding [18]. These findings suggest that while increased awareness is beneficial, deeper cultural shifts are required to dismantle menstrual taboos and encourage evidence-based practices.
Conclusion
The study concluded that educational attainment and the type of menstrual material used were significant factors in determining young female adults’ awareness of proper menstrual hygiene, with higher education levels and modern menstrual products correlating with increased awareness. Geographic location influenced awareness of menstrual practices but not hygiene routines, with rural areas showing slightly higher awareness levels. Despite these findings, there was no significant correlation between menstrual hygiene awareness and menstrual beliefs, highlighting the complexity of changing deep-seated cultural norms. These results underscore the need for targeted educational interventions and the promotion of modern menstrual products to enhance MHL and practices, ultimately improving menstrual health outcomes for young female adults.
Study limitations
Despite its significant findings, this study has several limitations. First, the study relied on self-reported data, which may be subject to response bias, as participants might have overestimated or underestimated their awareness of menstrual hygiene. Second, the study focused on a specific population, limiting the generalizability of the results to other regions or demographic groups with different cultural and socioeconomic backgrounds. Third, while the study examined the influence of education and geographic location, it did not account for other potential factors, such as access to menstrual hygiene products, exposure to health education programs, and family influence, which may have affected the respondents’ awareness levels. The study did not include a qualitative component, which could have provided deeper insights into the cultural and social factors influencing menstrual hygiene awareness. Future research should address these limitations by incorporating a more diverse sample, exploring additional influencing factors and utilizing mixed-method approaches to gain a more comprehensive understanding of menstrual health awareness.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of the Xavier Ateneo Research Ethics Board (Code: XU REC Package No. NSG-2024001285). Informed consent was obtained from all participants before their inclusion in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
conceptualization, data analysis and wrote the original draft: Izzy D. Abayabay, Chariefa Aaliyah C. Al Ali and Rodesa Shaira B. Cornito; Study design, data collection and revising the manuscript: Kyramae M. Alava, Yuri Benedict J. Autor, Ranieza Jazz R. Baltazar and Jasmine Kyle C. Casicas; Data interpretation and the literature review: Ma. Melevir Madelyn A. Castañares, Cristine M. Dulfo and Raenah Patrizia B. Dy; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all participants in this study for their time and cooperation.
References
- Thiyagarajan DK, Basit H, Jeanmonod R. Physiology, Menstrual Cycle. [Updated 2024 Sep 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. [Link]
- Sakhi R, Jalalzai S, Ahmadi Z, Almaszada R, Zarghoon FN, Mohammadi R, et al. Knowledge, beliefs, and practices related to menstruation among female students in Afghanistan. International Journal of Women’s Health. 2023; 15:1139-49. [DOI:10.2147/IJWH.S410660] [PMID]
- Odey GO, Amusile O, Oghenetejiri PO, David S, Adi A, Lucero-Prisno DE 3rd. Period during a pandemic: The neglected reality of Nigerian girls and women. Public Health in Practice. 2021; 2:100196. [DOI:10.1016/j.puhip.2021.100196] [PMID]
- Castro S, Czura K. Social norms and misinformation: Experimental evidence on learning about menstrual health management in rural Bangladesh. CESifo Working. 2021; 9081. [DOI:10.2139/ssrn.3848343]
- Sommer M, Caruso BA, Torondel B, Warren EC, Yamakoshi B, Haver J, et al. Menstrual hygiene management in schools: Midway progress update on the "MHM in Ten" 2014-2024 global agenda. Health Research Policy and Systems. 2021; 19(1):1. [DOI:10.1186/s12961-020-00669-8] [PMID]
- Nanjundeswaraswamy TS, Divakar S. Determination of sample size and sampling methods in applied research. Proceedings in Engineering Sciences. 2021; 3(1):25-32. [DOI:10.24874/PES03.01.003]
- Hennegan J, Nansubuga A, Akullo A, Smith C, Schwab KJ. The Menstrual Practices Questionnaire (MPQ): Development, elaboration, and implications for future research. Global Health Action. 2020; 13(1):1829402. [DOI:10.1080/16549716.2020.1829402] [PMID]
- Simkus J. What is an ANOVA test in statistics: Analysis of variance. Simply Psychology. 2023. [Link]
- Thukral S, Kováč Š, Paturu M. T-test. In: Eltorai AEM, Liu T, Kalva SP, editors. Cambridge: Academic Press; 2023. [DOI:10.1016/B978-0-12-823026-8.00104-8]
- Gnambs T. A brief note on the standard error of the Pearson correlation. Collabra: Psychology. 2023; 9(1):1-5. [DOI:10.1525/collabra.87615]
- Roy A, Paul P, Saha J, Barman B, Kapasia N, Chouhan P, et al. Prevalence and correlates of menstrual hygiene practices among young currently married women aged 15-24 years: An analysis from a nationally representative survey of India. European Journal of Contraception & Reproductive Health Care. 2020; 26(1):1-10. [DOI:10.1080/13625187.2020.1810227] [PMID]
- Parasuraman G, Vijay V, Balaji S, Nisha B, Dutta R, Jain T, et al. Impact of health education intervention on menstruation and its hygiene among urban school-going adolescent girls in Thiruvallur, Tamilnadu. Journal of Family Medicine and Primary Care. 2022; 11(9):5271-6. [DOI:10.4103/jfmpc.jfmpc_46_22] [PMID]
- Karjee S, Rahaman M, Biswas PC. Contextualizing the socioeconomic and spatial patterns of using menstrual hygienic methods among young women (15-24 years) in India: A cross-sectional study using the nationally representative survey. Clinical Epidemiology and Global Health. 2023; 20:101253. [DOI:10.1016/j.cegh.2023.101253]
- Deepa S, Agrawal T, Attokaran T, Fathima FN, Johnson AR. Awareness, perceptions and practices regarding menstruation and menstrual hygiene among students of a college in Bengaluru Urban district, South India: A cross-sectional study. International Journal of Community Medicine and Public Health. 2019; 6(3):1126-31. [DOI:10.18203/2394-6040.ijcmph20190597]
- Shannon AK, Melendez-Torres GJ, Hennegan J. How do women and girls experience menstrual health interventions in low- and middle-income countries? Insights from a systematic review and qualitative metasynthesis. Culture, Health & Sexuality. 2021; 23(5):624-43. [DOI:10.1080/13691058.2020.1718758] [PMID]
- Ritika M, Neha A, Dixita K. Study of menstrual hygiene practices among the women of reproductive age group in Sangrur Village, Pune-Maharashtra. Cardiometry. 2022; 1(25):422-5. [Link]
- Tshomo T, Gurung MS, Shah S, Gil-Cuesta J, Maes P, Wangdi R, et al. Menstrual hygiene management-knowledge, attitudes, and practices among female college students in Bhutan. Frontiers in Reproductive Health. 2021; 3:703978. [DOI:10.3389/frph.2021.703978] [PMID]
- Karout N. Knowledge and beliefs regarding menstruation among Saudi nursing students. Journal of Nursing Education and Practice. 2016; 6(1):23-9. [DOI:10.5430/jnep.v6n1p23]
Type of Study: Original Article |
Subject:
Community Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
