

Volume 13, Issue 2 (Spring 2025)
Iran J Health Sci 2025, 13(2): 145-154 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Faraji H, KHorasaniToroghi H, Mirzaei V. Investigating the Impact of Organizational Bullying on Employee’s Mental Health. Iran J Health Sci 2025; 13 (2) :145-154
URL: http://jhs.mazums.ac.ir/article-1-1012-en.html
URL: http://jhs.mazums.ac.ir/article-1-1012-en.html



Department of Management, Faculty of Humanities, Bojnourd Branch, Islamic Azad University, Bojnourd, Iran. , khorasanitoroghi@gmail.com
Keywords: Organizational bullying, Mental health, Depression, Physical reactions, Social functioning
Full-Text [PDF 905 kb]
(547 Downloads)
| Abstract (HTML) (1453 Views)
Full-Text: (323 Views)
Introduction
Workplace bullying has become a common and significant problem in modern workplaces that can inflict severe harm to employees and organizations [1]. Bullying is a harmful act carried out to hurt a perceived weak individual. Bullying can lead to short-term effects, such as physical harm, or long-term effects, such as anxiety, depression, and using addictive substances [2]. Organizational bullying not only harms employees but also affects the efficiency and performance of organizations, becoming a public concern for both governmental and non-governmental organizations [3]. Workplace bullying can spread if neglected; policymakers and managers should pay serious attention to it [4]. Workplace bullying increases stress and reduces performance [5].
Bullying in the workplace in public and private organizations has a detrimental effect on employees and threatens team spirit and cohesion, cooperation, participation, and empathy [6]. Threatening and disruptive workplace bullying promotes making mistakes. It contributes to adverse outcomes, which harm the client, lower worker morale and increase absenteeism, resulting in higher turnover rates or intention to quit for skilled workers. Employees exposed to bullying may face serious consequences, such as low self-esteem and a negative impact on organizational efficiency. Loneliness and social isolation are consequences of bullying [7]. The loneliness caused by bullying causes stress, anxiety, and other health problems for the victim [8].
Employees’ mental health is key to improving productivity and organizational efficiency. Organizations with employees with high mental health can achieve their goals and missions more effectively. However, workplaces where organizational bullying is prevalent can quickly become environments filled with stress, anxiety, depression and other mental disorders. Research shows that victims of organizational bullying often experience anxiety, sleep disorders, depression and reduced self-confidence. Victims of organizational bullying usually experience high levels of anxiety and stress. This ongoing stress can lead to anxiety disorders that require psychological and medical treatments [9].
Repeated exposure to bullying can lead to severe depression. Victims often feel worthless, hopeless and depressed, which can affect their personal and professional lives [10].
In extreme cases, organizational bullying can lead to suicidal thoughts or self-harming behaviors. Victims who see no escape from their situation turn to final and desperate solutions [9].
According to Rosander and Blomberg (2019), 19% of employees have significantly experienced bullying, negatively affecting their health and well-being, with 7% enduring severe or continuous bullying [11]. While most studies on organizational bullying focus on mental health consequences like anxiety or depression, some consider mental health problems as pre-existing risk factors [12]. Several studies have examined the relationship between workplace bullying and its adverse impacts on employees. Lo Presti et al. found that bullying was associated with negative physical symptoms, with anxiety and depression serving as mediators in this relationship [13]. Nauman et al. revealed that workplace bullying increases occupational anxiety and insomnia, which in turn reduces employees’ life satisfaction [14]. Lee et al. showed that bullying leads to higher cortisol levels, the stress hormone, which can result in physical problems such as weight gain, diabetes and other metabolic disorders [15]. Hui et al. demonstrated that bullying could cause a range of physical problems, including headaches, muscle pain, digestive issues and high blood pressure [10]. Török et al. found that bullying by leaders was linked to more severe depressive symptoms [16]. Finally, Rodell et al. emphasized that bullying could significantly increase depression levels and have long-term effects on mental health [17].
This research was conducted to bridge the gaps in the existing literature regarding organizational bullying and its impact on the mental health of employees, particularly in government organizations with ethnic diversity. Although many studies have examined bullying in work environments, there is a lack of studies, especially regarding the psychological effects of this phenomenon on employees in government organizations with specific cultural and social characteristics, such as municipalities. Furthermore, most research has focused on the physical and behavioral aspects of bullying, with less attention paid to its effects on mental health and specific issues such as anxiety, depression and sleep disorders, which is the novelty of this study.
Therefore, this study examines the relationship between organizational bullying and the mental health of employees in the municipality of Bojnourd City, Iran, aiming to fill this research gap and analyze its impact on various aspects of employees’ mental health, such as anxiety, depression, sleep disorders, and social functioning. The importance of this research lies in its broader context of organizational psychology and mental health, particularly in workplaces with ethnic and cultural diversity. Given the growing attention to mental health in workplaces, this research can serve as a foundation for designing strategies and managerial policies to reduce bullying and improve employees’ mental health in government organizations.
Material and Methods
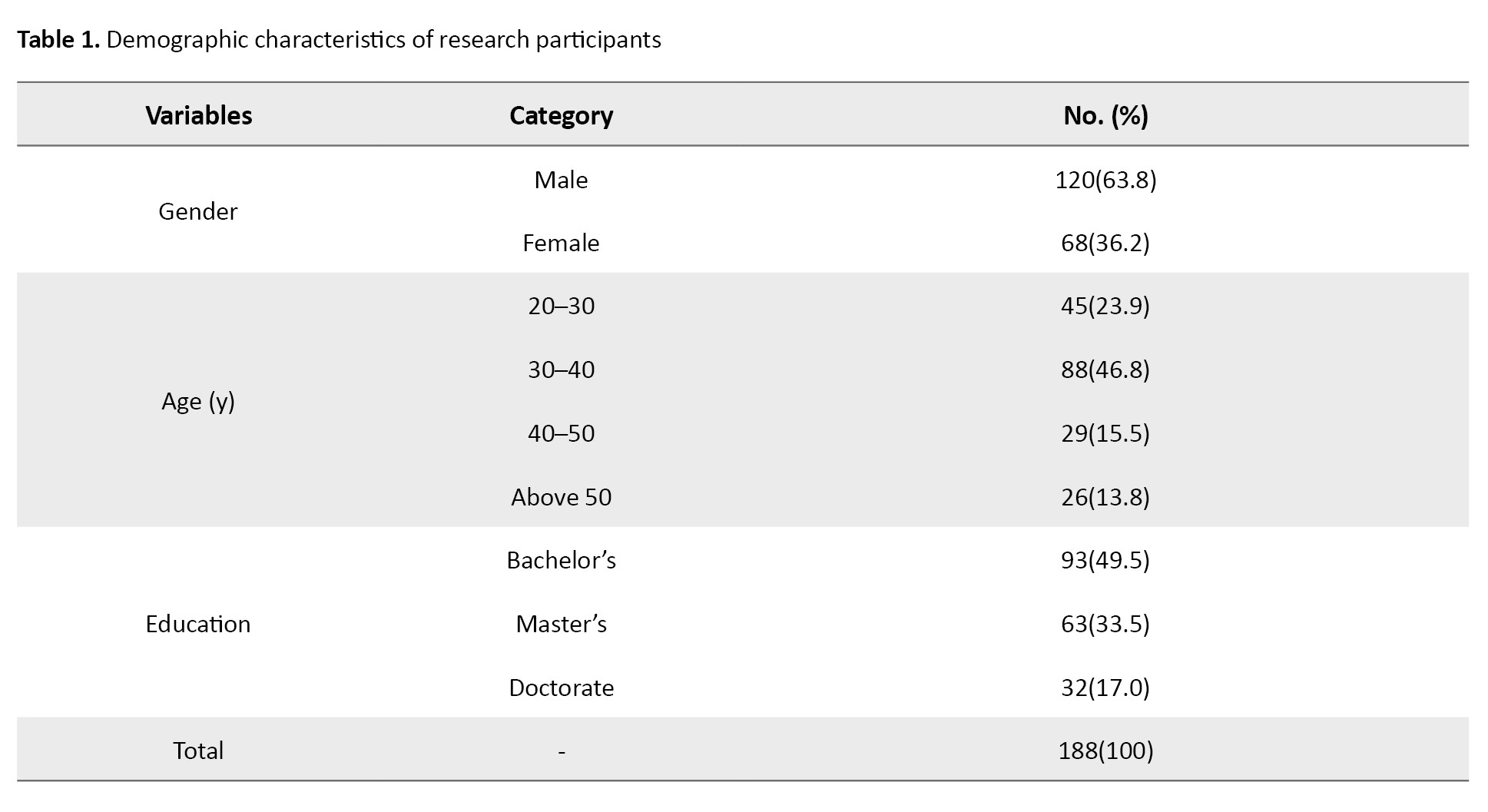
This research is applied in terms of purpose and descriptive-correlational regarding information gathering. The statistical population comprised the employees of Bojnourd Municipality with at least 10 years of work experience who had encountered workplace bullying during their service. According to statistics, the population size is 370. Using the Cochran formula, 188 individuals were selected as the sample size through simple random sampling. The inclusion criteria were at least 10 years of experience working in Bojnourd municipality and holding a bachelor’s degree or higher in Management, Educational Sciences, or Psychology. The exclusion criteria were unwillingness to participate in the study or failure to complete the questionnaires. The study tools used were self-assessment questionnaires completed by the participants. The validity of these questionnaires was assessed before the study to ensure their suitability for the target population. The Leymann workplace bullying questionnaire (1996) was employed to determine the variable of workplace bullying, which includes 45 types of bullying behaviors [18]. This scale is categorized into five dimensions: questions 1–11 refer to “threatening communication behaviors,” questions 12–16 to “threatening social relationship behaviors,” questions 17–31 to “threatening personal reputation behaviors,” questions 32–40 to “threatening occupational position behaviors,” and questions 41–45 to “threatening physical health behaviors.” Scoring for this questionnaire is based on a 5-point Likert scale: 5 points for “every day,” 4 points for “several times a week,” 3 points for “several times a month,” 2 points for “several times a year,” and 1 point for “never.” This scale has been used in several studies, and its reliability and validity have been evaluated. In Şahin et al.’s study [19], the reliability scores were 0.87 for threatening communication behaviors, 0.71 for threatening social relationship behaviors, 0.90 for threatening personal reputation behaviors, 0.89 for threatening occupational position behaviors, and 0.74 for threatening physical health behaviors, with an overall reliability score of 0.95. For the mental health variable, the Goldberg and Hillier mental health questionnaire (1979) was used [20]. Questions 1–7 address physical symptoms, 8–14 focus, and 22–28 relate to depression. Scoring is as follows: “Not at all” scores 0, “no more than usual” scores 1, “more than usual” scores 2, and “much more than usual” scores 3. A score of 6 or higher on any subscale or a total score of 22 or higher indicates pathological symptoms. This tool has been validated in various studies and has demonstrated good reliability. Demographic information (such as age, gender, and education level) was collected to analyze the impact of demographic variables on the study variables. The questionnaires were administered in person and distributed as hard copies among Bojnourd Municipality employees. Before distribution, clear instructions on how to complete the questionnaires were provided to the participants. To ensure standardized data collection, the questionnaires were designed based on standardized measurement tools and validated scales from previous research, and their validity and reliability were assessed. All questionnaires were distributed in person under uniform conditions among Bojnourd Municipality employees to prevent discrepancies arising from different data collection methods. Before completing the questionnaire, the respondents were provided with necessary explanations regarding the research objectives and response guidelines to avoid misinterpretation of the questions. After data collection, an initial review was conducted to identify incomplete or inconsistent responses, ensuring the quality of the collected data. Ethical considerations were adhered to, including obtaining informed consent from participants, ensuring confidentiality of information, and providing adequate explanations about the study’s objectives. Data analysis was conducted using SPSS software, version 22 and structural equation modeling (SEM) was applied for statistical analysis.
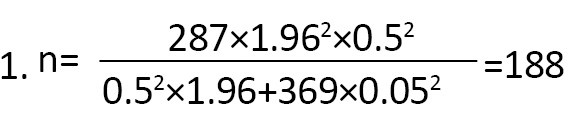
Cochran formula (Equation 1) was used to determine the sample size of the research, considering N: Statistical population size, n: Sample size, e: Error coefficient (0.05), δ: Standard deviation of the sample (0.5) and Z.1.96 is the standard normal random variable value (1.96).
Results
Description of demographic variablesto better understand the nature of the study population before statistical data analysis, it is essential to describe these data. Table 1 presents the demographic characteristics of the research participants.
The SEM using the partial least squares (PLS) approach consists of the following three main stages:
Measurement model fit (relationships between indicators and latent variables)
This model is evaluated using factor loadings’ significance, composite reliability, average variance extracted (AVE) and the Fornell-Larcker matrix.
Structural model fit (relationships between latent variables)
This model is assessed using the coefficient of determination (R²), predictive relevance (Q²), path coefficients (beta) and their significance (t values).
Overall model fit (combination of measurement and structural models)
The goodness of fit (GOF) index is the only criterion calculated in the SEM approach using PLS.
Measurement model fit (relationships between indicators and latent variables)
Confirmatory factor analysis (factor loadings and t values)
The measurement model focuses on and assesses the relationships between observed and latent variables. The evaluation of this model includes composite reliability to evaluate internal consistency, indicator reliability, and the AVE to evaluate convergent validity. Additionally, the Fornell-Larcker criterion is used to assess discriminant validity.
Table 2 presents the descriptive indicators of the research variables, including the original sample (O), sample Mean±SD, t statistics and significance values of P.
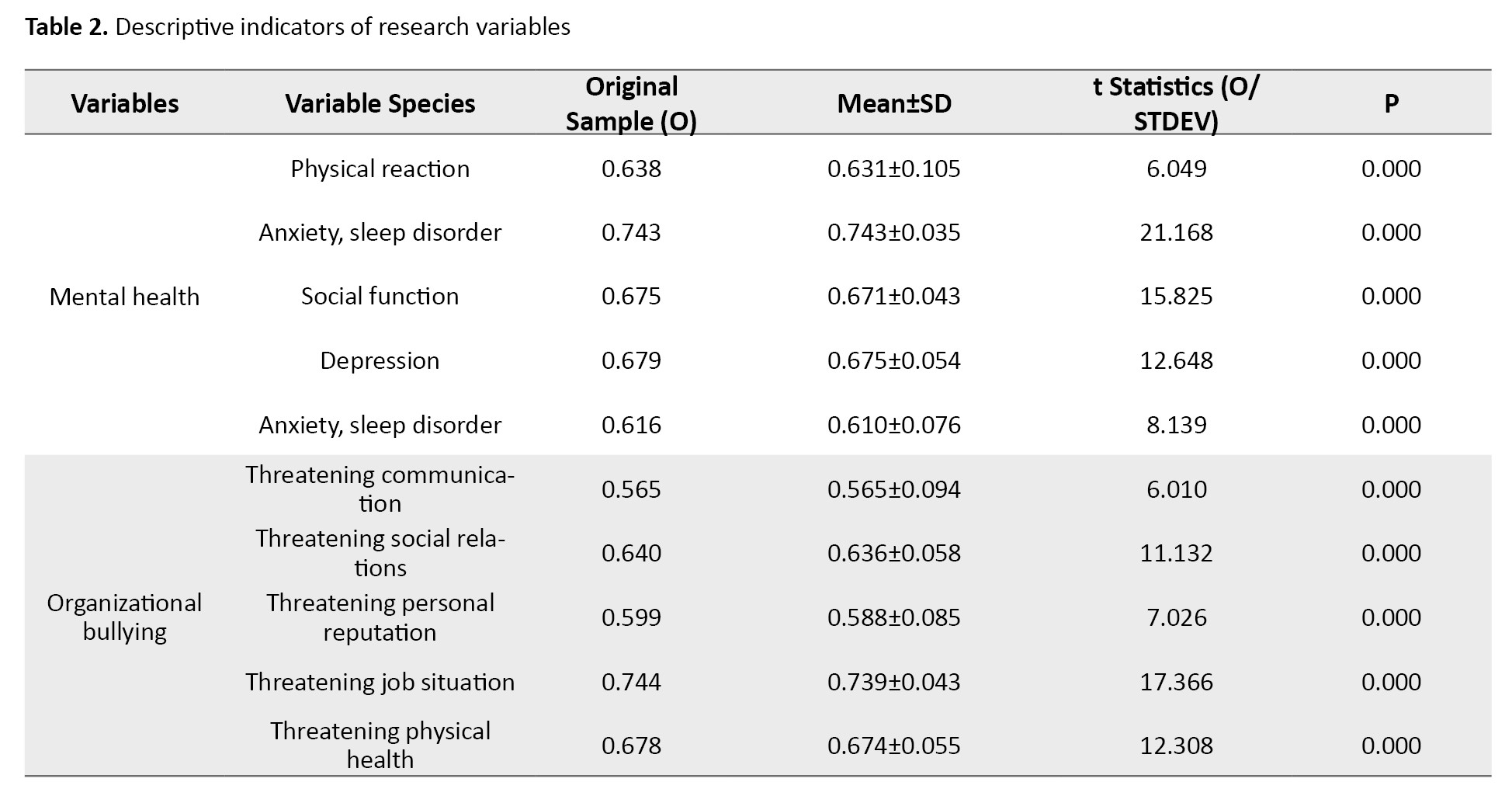
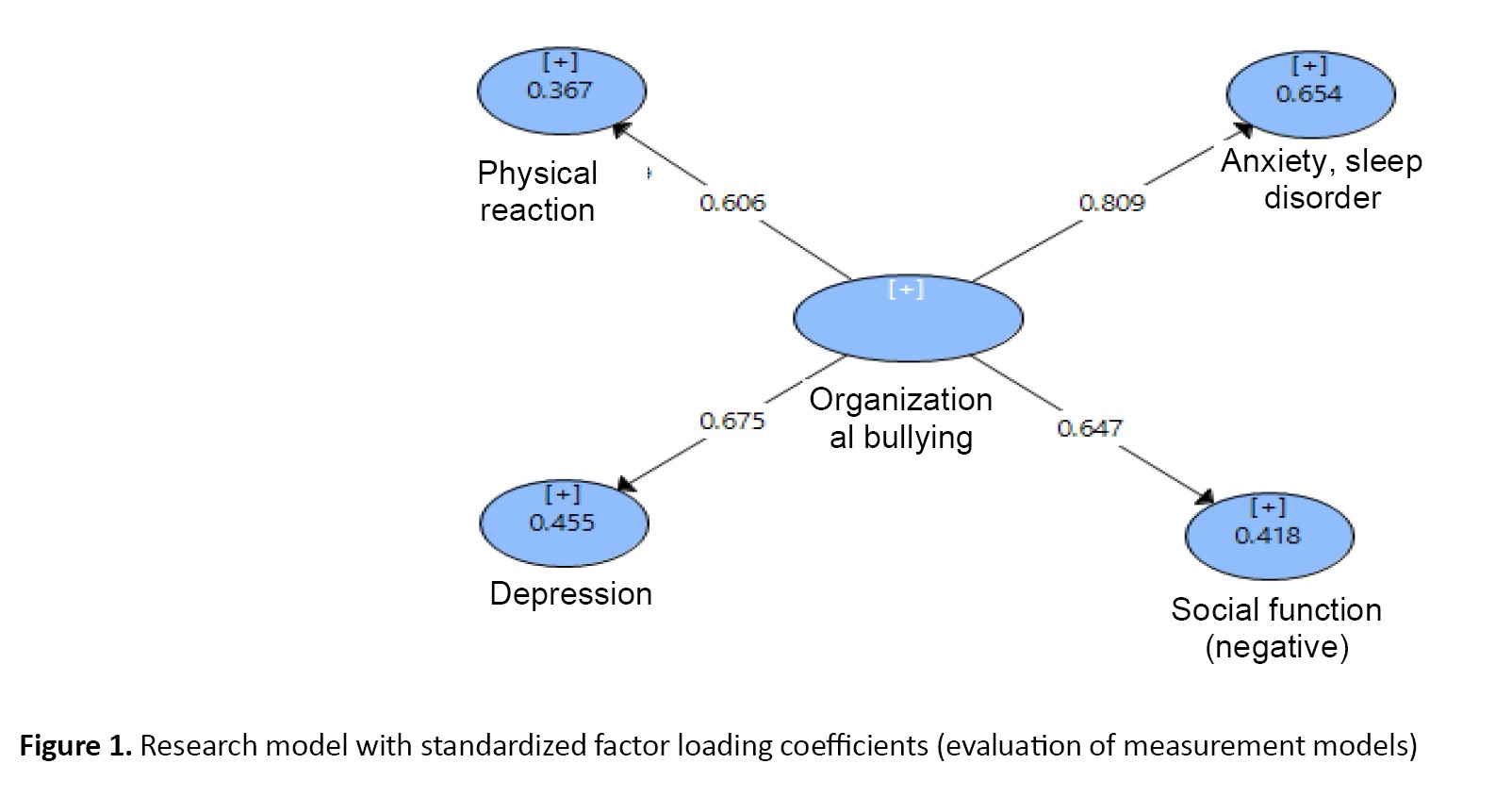
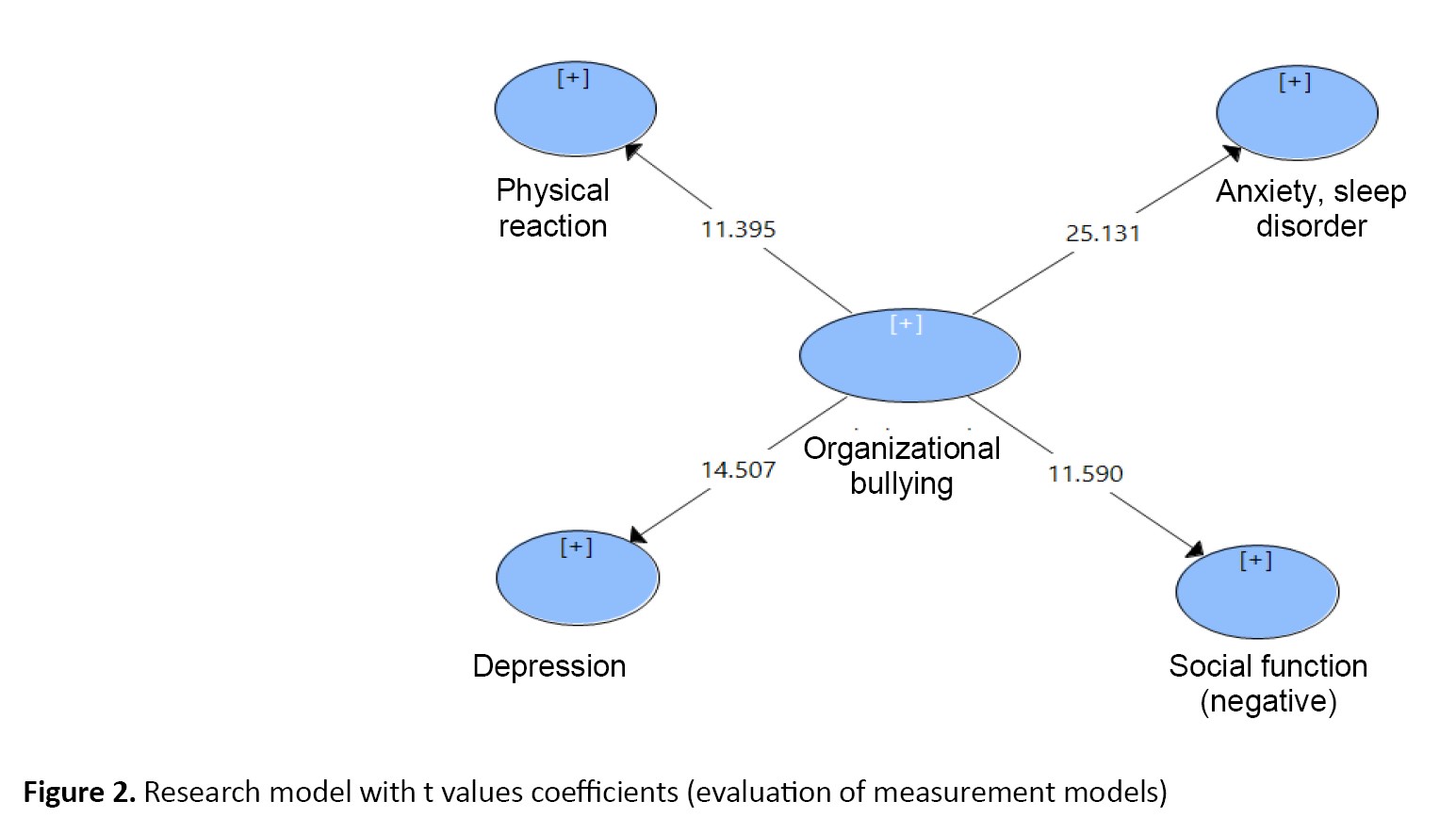
Table 2 presents the output of factor loadings analysis using the PLS method and examines the relationships between variables and components. The estimated value indicates the strength and direction of the impact of each component (factor loadings) on its corresponding variable in the bootstrapping analysis. A significance level of <0.05 and a t>1.96 indicate that the constructs of each research variable are well explained by the observed components, demonstrating one of the acceptable fit parameters of the measurement model (Figure 1 and 2).
Examination of the measurement model (outer model)
Convergent validity (AVE)
This index shows the degree of correlation of a structure with its indicators. For this index, a minimum value of 0.5 is considered, which means that the desired hidden variable explains at least 50% of the variance of its observables [21]. Table 3 shows the fit indices of the measurement models.
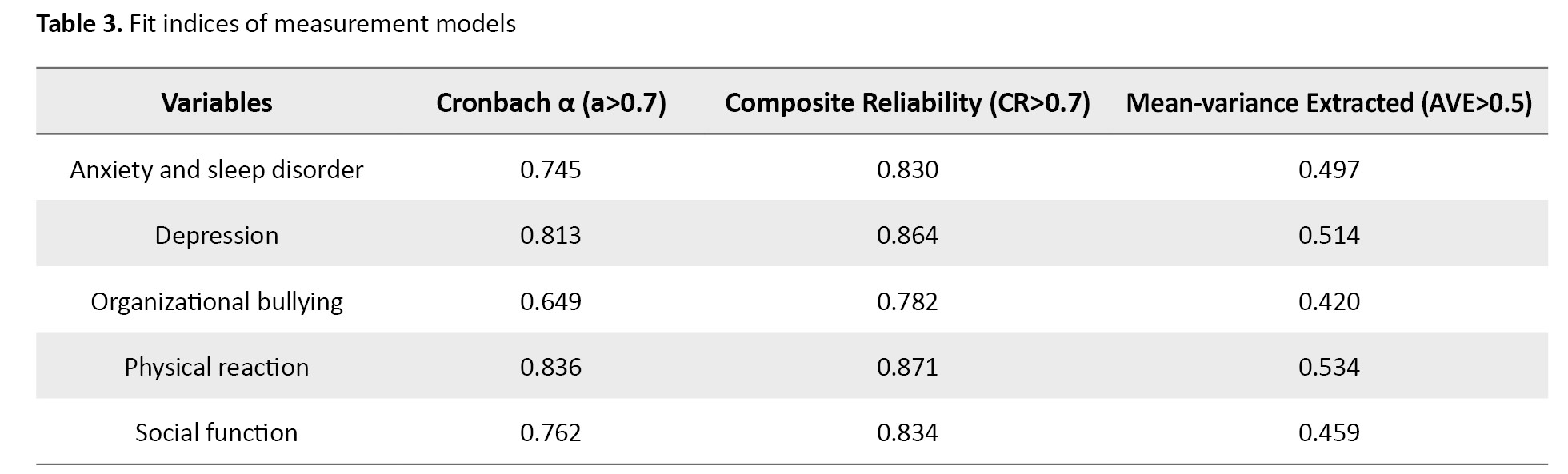
The combined reliability coefficient and Cronbach α coefficient are at a very favorable level and the AVE of the constructs is also favorable.
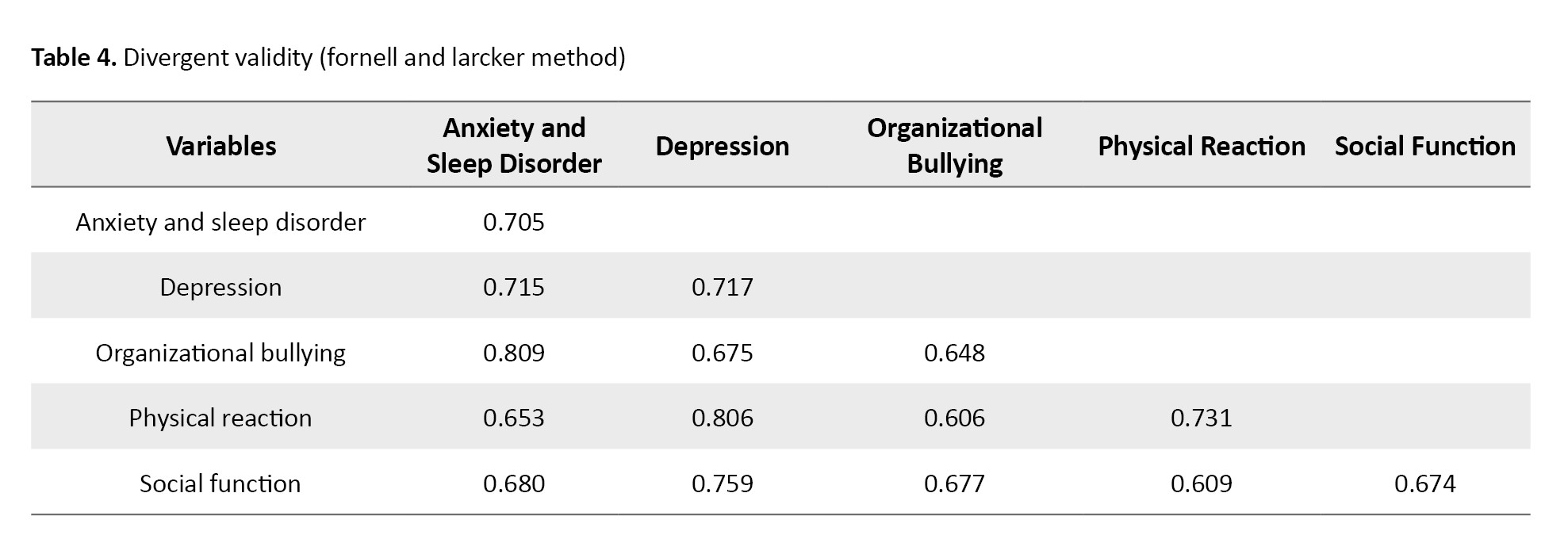
Divergent validity (fornell and larcker method)
Another vital criterion is divergent validity; divergent validity complements convergent validity, which is measured through the Fornell-Larker test (Table 4).
Structural model fit (relationships between latent variables)
Coefficient of determination index (R2) Endogenous Variables
The coefficient R2 indicates the effect of an exogenous variable on an endogenous variable, and three values of 0.19, 0.33 and 0.67 are considered the criteria for weak, medium and strong values of R2. The higher R2 is related to the endogenous structures of a model, the better the fit of the model (Table 5).
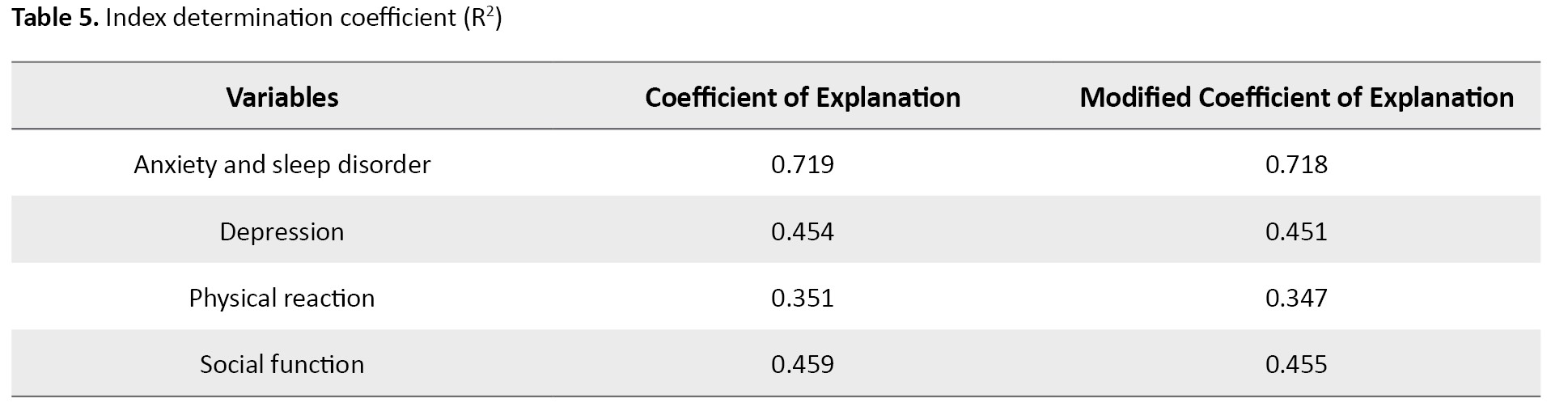
The determination coefficients show that more than 70% of the changes are related to the variable of anxiety and sleep disorder. More than 45% of the changes are associated with the variable of depression symptomsand explain it. The rest of the changes in these variables are related to physical health, social functioning and other factors and components not considered in the model and research.
Predictive correlation index Q2
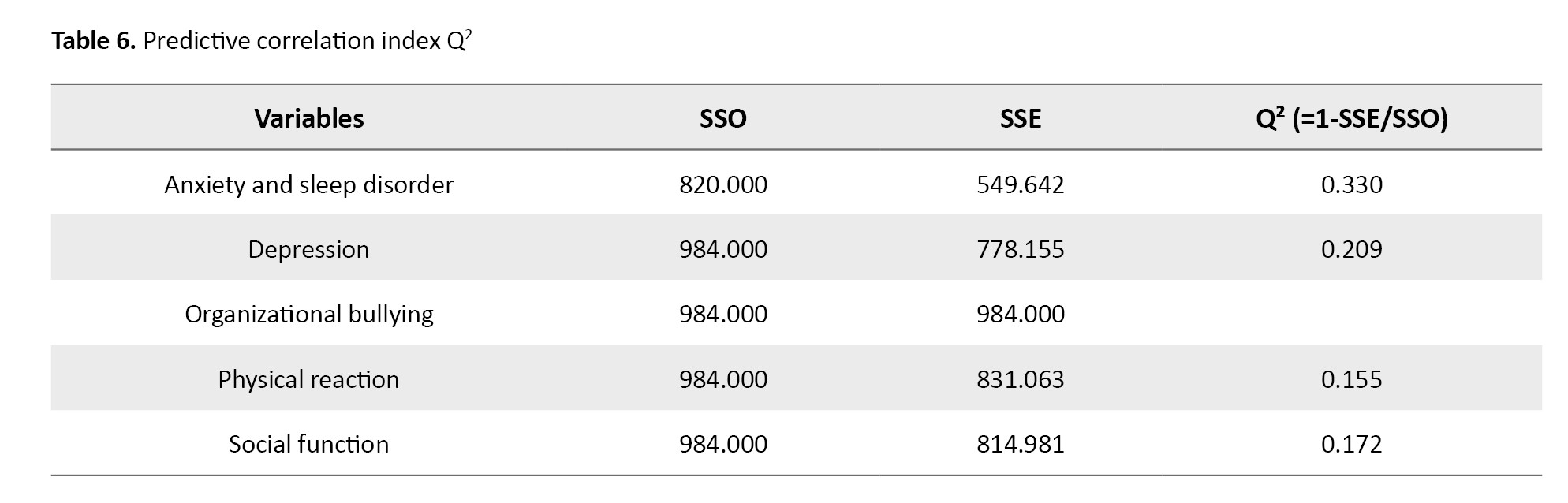
The criterion Q2 (Stone-Geisser) determines the model’s predictive power in the dependent variables. According to their belief, the models with an acceptable structural fit should be able to predict the indicators related to the endogenous structures of the model. Value Q2>0 indicates the model has a predictive fit for a given endogenous construct. On the other hand, zero and lower values indicate the lack of predictive fit. It determines three values: 0.02, 0.15 and 0.35, as low, medium and strong predictive power.
According to the Table 6, the prediction value Q2 of the model regarding the mentioned variables has moderate and appropriate power.
Overall model fit (combination of measurement and structural models)
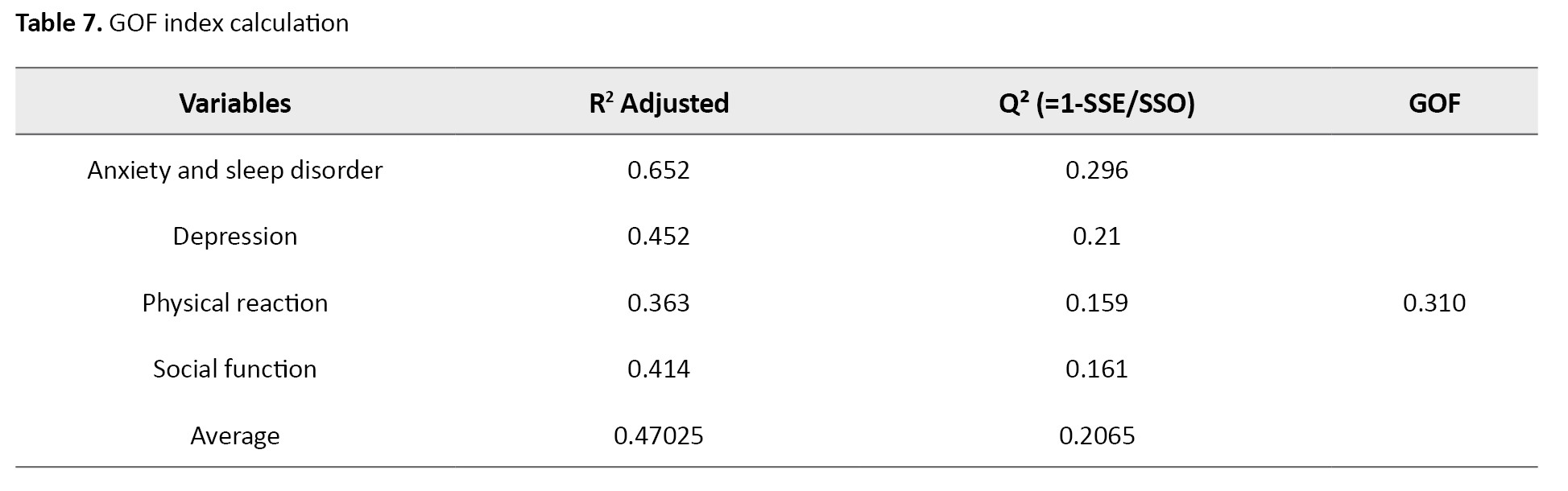
After evaluating the measurement and structural models, the overall model (the sum of the measurement and structural models) should also be examined. For this purpose, Tenenhaus et al. introduced the GOF index [22]. The Equation 2 calculates this index and three values of 0.01, 0.25 and 0.36 are considered weak, medium and strong. The closer the value of this person is to 1, the stronger the overall model.

As seen in the Table 7, the value of the GOF index of the model is equal to 0.310, which means that the model is relatively suitable.
Examining research hypotheses
Discussion
The results of this study showed that bullying in the workplace has significant negative effects on the mental health of employees. Based on the fact that the path coefficient in the first hypothesis is estimated at 0.809, with a significance level of 0.000 and a t=25.131, which is both <0.05 and >1.96, this path coefficient is significant at the 0.05 error level (Table 8).
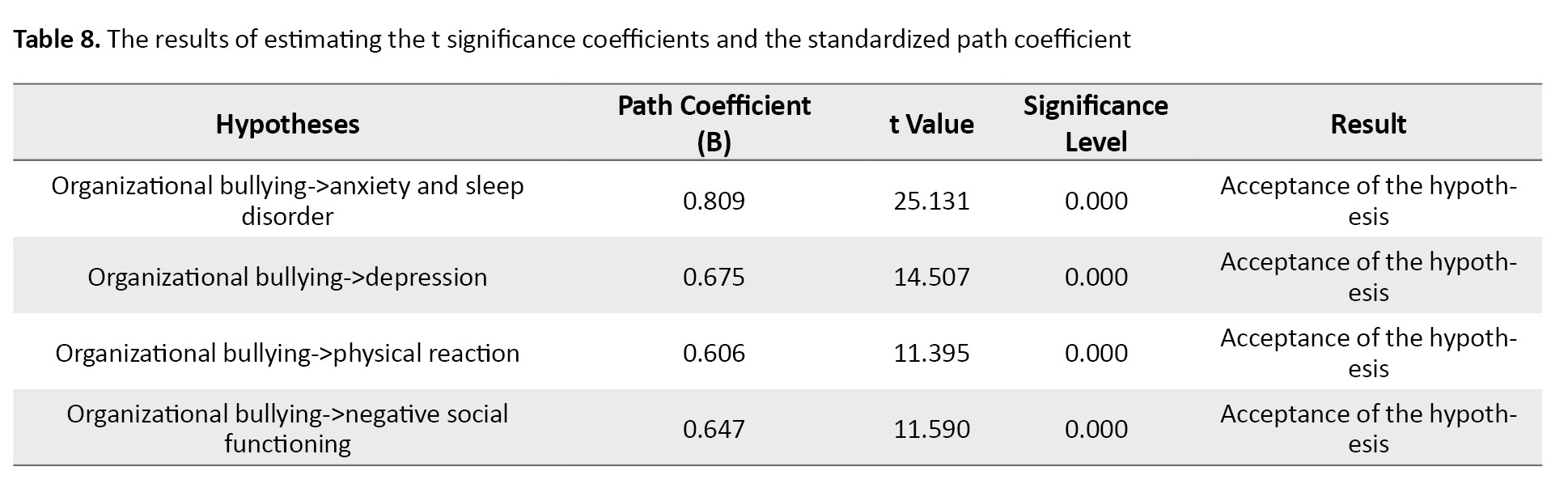
Therefore, with 95% confidence, the first hypothesis of the study, which suggests that organizational bullying impacts anxiety and sleep disorders, is accepted. Nauman et al. (2019) demonstrated that workplace bullying leads to increased job-related anxiety and insomnia, which subsequently reduces employees’ life satisfaction. The findings of hypothesis 1 align with these results, as this study also shows that workplace and environmental threats stemming from bullying lead to job anxiety and poor sleep quality. These similarities, particularly regarding the psychological effects of bullying and its impact on employees’ mental health, reveal significant consistency with Nauman et al. research [14]. Similarly, Lo Presti et al. highlighted the association between workplace bullying and anxiety and depression, identifying these two variables as mediators in the relationship [13].
Consistent with this study, the findings of hypothesis 1 reveal that workplace bullying directly contributes to the onset of depression. Specifically, the significant relationship between bullying, depression and anxiety in this research mirrors the findings of Lo Presti et al. emphasizing the direct negative effects of bullying behaviors on employees’ mental health. The innovation of this research lies in its focus on the types of bullying threats and their specific effects on mental health. Notably, this hypothesis examines the impact of bullying in distinct areas, such as job-related threats, social threats, and physical health threats—dimensions that have received less attention in some prior studies. These findings, supported by up-to-date data and a broad sample population, provide a more comprehensive perspective on the effects of workplace bullying. This detailed analysis clarifies the relationships between bullying and specific psychological outcomes, such as anxiety and sleep disorders, with greater precision. It can be explained that bullying in the workplace has significant negative effects on employees’ mental health, especially in increasing the level of anxiety and sleep disorders. This relationship can be explained through various mechanisms such as increased stress, decreased sense of control over job tasks and additional cognitive load. In particular, the constant stress caused by bullying can lead to intrusive thoughts and nightly worries, which in turn lead to insomnia and increased anxiety. Based on the fact that the path coefficient in the second hypothesis is estimated to be 0.675 and considering the significance level of 0.000 and the significance value of 14.507, which are both <0.05 and >1.96, this path coefficient is significant at the 0.05 error level. Therefore, with 95% confidence, it can be stated that the second hypothesis of the research, which suggests that organizational bullying affects depression, is accepted. Török et al. in a study conducted on 2478 employees in Denmark, found that individuals exposed to bullying by their leaders experienced more severe symptoms of depression [16]. The findings of the second hypothesis in this study similarly indicate that organizational bullying can directly influence the severity of depression, aligning with the results of this research. Additionally, Rodell et al. emphasized in their study that bullying can significantly increase the level of depression and have long-term effects on employees’ mental health [17].
The results of this hypothesis also confirm this impact, showing a significant relationship between organizational bullying and depression. According to Nielsen and Einarsen, exposure to systematic and prolonged aggressive behaviors negatively impacts the individual, causing cognitive activation and subsequent physiological activation that, if prolonged, damage health and well-being. In particular, given that each subject can have different consequences and show different reactions, leading to changes in cognitive-emotional balance (such as depression, anxiety, obsessions, panic attacks, emotional numbness) as well as in psychosomatic balance (such as digestive disorders) [23]. Considering that the path coefficient in the fourth hypothesis is estimated to be 0.647 and the significance level is 0.000, with a significance value of 11.590, which is <0.05 and >1.96, it can be concluded that this path coefficient is significant at the 0.05 error level. Therefore, with 95% confidence, the fourth hypothesis of the research, which suggests that organizational bullying negatively affects social functioning, is accepted. The results of this hypothesis are consistent with the research of Einarsen and Raknes [24].
This study focuses on the impact of bullying on reducing social interactions and increasing social isolation in the workplace. The results show that bullying victims are less likely to engage in positive interactions with their colleagues and tend to avoid social activities in the workplace. Your research also shows a similar impact on social functioning but with a focus on more specific outcomes. The innovation of this study lies in the fact that, unlike previous studies, which mainly referenced the reduction of interactions or feelings of isolation, our research specifically examines the functional consequences resulting from the reduction of social interactions. In explaining this relationship, it is stated that workplace bullying has significant effects on employees’ negative social functioning. Victims of bullying often suffer from a decrease in self-confidence and social activities, which can lead to a decrease in positive interactions with colleagues and a decrease in cooperation in the workplace. Bullying behaviors not only weaken professional and social relationships but also affect employees’ sense of belonging and motivation. These conditions can decrease the overall productivity and efficiency of the organization. Therefore, creating supportive work environments, formulating effective policies to deal with bullying, and providing training and support programs to strengthen employees’ social skills can help to improve social functioning and promote their mental and professional health.
Conclusion
The results of this research emphasize the need to pay attention to employees’ mental health and to adopt preventive measures against bullying in the workplace. To reduce the negative impacts of organizational bullying, managers should implement practical and effective actions to support employees and improve working conditions. Therefore, with the results obtained from this research, managers should take practical and effective measures to reduce the adverse effects of organizational bullying on the mental health of Bojnourd Municipality employees. It is suggested that clear and specific anti-bullying policies be formulated and implemented and confidential reporting systems be designed to facilitate complaints. Also, holding training courses to increase the awareness and communication skills of employees and managers, creating a supportive work environment encouraging positive behaviors and providing counseling and psychological support to victims of bullying can help improve employees’ mental health and the quality of the work environment. These measures will generally prevent bullying and improve the quality of interactions and mental health in the workplace.
Study limitations
This study focuses solely on the employees of the Bojnourd Municipality. Therefore, the results may not be fully generalizable to other organizations or regions. Due to time limitations, this research has not examined the long-term effects of organizational bullying on employees’ mental health. It may only cover short-term or medium-term impacts. In this study, self-report methods (such as questionnaires and interviews) were used for data collection, and these methods are liable to challenges such as response bias or lack of honesty, which can affect the accuracy of the results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Bojnourd Branch, Bojnourd, Iran (Code: IR.IAU.BOJNOURD.REC.1403.013).
Funding
The paper was extracted from the PhD thesis of Hosein Faraji, approved by Islamic Azad University of Bojnourd, Bojnourd, Iran.
Authors contributions
Conceptualization and supervision: Hamed Khorasani Toroghi and Vahid Mirzaei; Methodology: Hamed Khorasani Toroghi and Hossein Faraji; Data collection: Vahid Mirzaei and Hamed Khorasani Toroghi; Data analysis: Vahid Mirzaei and Hossein Faraji; Funding acquisition and resources: Hamed Khorasani Toroghi and Hossein Faraji; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the Student Research Committee of the Islamic Azad University of Bojnourd for supporting this research.
References
Workplace bullying has become a common and significant problem in modern workplaces that can inflict severe harm to employees and organizations [1]. Bullying is a harmful act carried out to hurt a perceived weak individual. Bullying can lead to short-term effects, such as physical harm, or long-term effects, such as anxiety, depression, and using addictive substances [2]. Organizational bullying not only harms employees but also affects the efficiency and performance of organizations, becoming a public concern for both governmental and non-governmental organizations [3]. Workplace bullying can spread if neglected; policymakers and managers should pay serious attention to it [4]. Workplace bullying increases stress and reduces performance [5].
Bullying in the workplace in public and private organizations has a detrimental effect on employees and threatens team spirit and cohesion, cooperation, participation, and empathy [6]. Threatening and disruptive workplace bullying promotes making mistakes. It contributes to adverse outcomes, which harm the client, lower worker morale and increase absenteeism, resulting in higher turnover rates or intention to quit for skilled workers. Employees exposed to bullying may face serious consequences, such as low self-esteem and a negative impact on organizational efficiency. Loneliness and social isolation are consequences of bullying [7]. The loneliness caused by bullying causes stress, anxiety, and other health problems for the victim [8].
Employees’ mental health is key to improving productivity and organizational efficiency. Organizations with employees with high mental health can achieve their goals and missions more effectively. However, workplaces where organizational bullying is prevalent can quickly become environments filled with stress, anxiety, depression and other mental disorders. Research shows that victims of organizational bullying often experience anxiety, sleep disorders, depression and reduced self-confidence. Victims of organizational bullying usually experience high levels of anxiety and stress. This ongoing stress can lead to anxiety disorders that require psychological and medical treatments [9].
Repeated exposure to bullying can lead to severe depression. Victims often feel worthless, hopeless and depressed, which can affect their personal and professional lives [10].
In extreme cases, organizational bullying can lead to suicidal thoughts or self-harming behaviors. Victims who see no escape from their situation turn to final and desperate solutions [9].
According to Rosander and Blomberg (2019), 19% of employees have significantly experienced bullying, negatively affecting their health and well-being, with 7% enduring severe or continuous bullying [11]. While most studies on organizational bullying focus on mental health consequences like anxiety or depression, some consider mental health problems as pre-existing risk factors [12]. Several studies have examined the relationship between workplace bullying and its adverse impacts on employees. Lo Presti et al. found that bullying was associated with negative physical symptoms, with anxiety and depression serving as mediators in this relationship [13]. Nauman et al. revealed that workplace bullying increases occupational anxiety and insomnia, which in turn reduces employees’ life satisfaction [14]. Lee et al. showed that bullying leads to higher cortisol levels, the stress hormone, which can result in physical problems such as weight gain, diabetes and other metabolic disorders [15]. Hui et al. demonstrated that bullying could cause a range of physical problems, including headaches, muscle pain, digestive issues and high blood pressure [10]. Török et al. found that bullying by leaders was linked to more severe depressive symptoms [16]. Finally, Rodell et al. emphasized that bullying could significantly increase depression levels and have long-term effects on mental health [17].
This research was conducted to bridge the gaps in the existing literature regarding organizational bullying and its impact on the mental health of employees, particularly in government organizations with ethnic diversity. Although many studies have examined bullying in work environments, there is a lack of studies, especially regarding the psychological effects of this phenomenon on employees in government organizations with specific cultural and social characteristics, such as municipalities. Furthermore, most research has focused on the physical and behavioral aspects of bullying, with less attention paid to its effects on mental health and specific issues such as anxiety, depression and sleep disorders, which is the novelty of this study.
Therefore, this study examines the relationship between organizational bullying and the mental health of employees in the municipality of Bojnourd City, Iran, aiming to fill this research gap and analyze its impact on various aspects of employees’ mental health, such as anxiety, depression, sleep disorders, and social functioning. The importance of this research lies in its broader context of organizational psychology and mental health, particularly in workplaces with ethnic and cultural diversity. Given the growing attention to mental health in workplaces, this research can serve as a foundation for designing strategies and managerial policies to reduce bullying and improve employees’ mental health in government organizations.
Material and Methods
This research is applied in terms of purpose and descriptive-correlational regarding information gathering. The statistical population comprised the employees of Bojnourd Municipality with at least 10 years of work experience who had encountered workplace bullying during their service. According to statistics, the population size is 370. Using the Cochran formula, 188 individuals were selected as the sample size through simple random sampling. The inclusion criteria were at least 10 years of experience working in Bojnourd municipality and holding a bachelor’s degree or higher in Management, Educational Sciences, or Psychology. The exclusion criteria were unwillingness to participate in the study or failure to complete the questionnaires. The study tools used were self-assessment questionnaires completed by the participants. The validity of these questionnaires was assessed before the study to ensure their suitability for the target population. The Leymann workplace bullying questionnaire (1996) was employed to determine the variable of workplace bullying, which includes 45 types of bullying behaviors [18]. This scale is categorized into five dimensions: questions 1–11 refer to “threatening communication behaviors,” questions 12–16 to “threatening social relationship behaviors,” questions 17–31 to “threatening personal reputation behaviors,” questions 32–40 to “threatening occupational position behaviors,” and questions 41–45 to “threatening physical health behaviors.” Scoring for this questionnaire is based on a 5-point Likert scale: 5 points for “every day,” 4 points for “several times a week,” 3 points for “several times a month,” 2 points for “several times a year,” and 1 point for “never.” This scale has been used in several studies, and its reliability and validity have been evaluated. In Şahin et al.’s study [19], the reliability scores were 0.87 for threatening communication behaviors, 0.71 for threatening social relationship behaviors, 0.90 for threatening personal reputation behaviors, 0.89 for threatening occupational position behaviors, and 0.74 for threatening physical health behaviors, with an overall reliability score of 0.95. For the mental health variable, the Goldberg and Hillier mental health questionnaire (1979) was used [20]. Questions 1–7 address physical symptoms, 8–14 focus, and 22–28 relate to depression. Scoring is as follows: “Not at all” scores 0, “no more than usual” scores 1, “more than usual” scores 2, and “much more than usual” scores 3. A score of 6 or higher on any subscale or a total score of 22 or higher indicates pathological symptoms. This tool has been validated in various studies and has demonstrated good reliability. Demographic information (such as age, gender, and education level) was collected to analyze the impact of demographic variables on the study variables. The questionnaires were administered in person and distributed as hard copies among Bojnourd Municipality employees. Before distribution, clear instructions on how to complete the questionnaires were provided to the participants. To ensure standardized data collection, the questionnaires were designed based on standardized measurement tools and validated scales from previous research, and their validity and reliability were assessed. All questionnaires were distributed in person under uniform conditions among Bojnourd Municipality employees to prevent discrepancies arising from different data collection methods. Before completing the questionnaire, the respondents were provided with necessary explanations regarding the research objectives and response guidelines to avoid misinterpretation of the questions. After data collection, an initial review was conducted to identify incomplete or inconsistent responses, ensuring the quality of the collected data. Ethical considerations were adhered to, including obtaining informed consent from participants, ensuring confidentiality of information, and providing adequate explanations about the study’s objectives. Data analysis was conducted using SPSS software, version 22 and structural equation modeling (SEM) was applied for statistical analysis.
Cochran formula (Equation 1) was used to determine the sample size of the research, considering N: Statistical population size, n: Sample size, e: Error coefficient (0.05), δ: Standard deviation of the sample (0.5) and Z.1.96 is the standard normal random variable value (1.96).
Results
Description of demographic variablesto better understand the nature of the study population before statistical data analysis, it is essential to describe these data. Table 1 presents the demographic characteristics of the research participants.
The SEM using the partial least squares (PLS) approach consists of the following three main stages:
Measurement model fit (relationships between indicators and latent variables)
This model is evaluated using factor loadings’ significance, composite reliability, average variance extracted (AVE) and the Fornell-Larcker matrix.
Structural model fit (relationships between latent variables)
This model is assessed using the coefficient of determination (R²), predictive relevance (Q²), path coefficients (beta) and their significance (t values).
Overall model fit (combination of measurement and structural models)
The goodness of fit (GOF) index is the only criterion calculated in the SEM approach using PLS.
Measurement model fit (relationships between indicators and latent variables)
Confirmatory factor analysis (factor loadings and t values)
The measurement model focuses on and assesses the relationships between observed and latent variables. The evaluation of this model includes composite reliability to evaluate internal consistency, indicator reliability, and the AVE to evaluate convergent validity. Additionally, the Fornell-Larcker criterion is used to assess discriminant validity.
Table 2 presents the descriptive indicators of the research variables, including the original sample (O), sample Mean±SD, t statistics and significance values of P.
Table 2 presents the output of factor loadings analysis using the PLS method and examines the relationships between variables and components. The estimated value indicates the strength and direction of the impact of each component (factor loadings) on its corresponding variable in the bootstrapping analysis. A significance level of <0.05 and a t>1.96 indicate that the constructs of each research variable are well explained by the observed components, demonstrating one of the acceptable fit parameters of the measurement model (Figure 1 and 2).
Examination of the measurement model (outer model)
Convergent validity (AVE)
This index shows the degree of correlation of a structure with its indicators. For this index, a minimum value of 0.5 is considered, which means that the desired hidden variable explains at least 50% of the variance of its observables [21]. Table 3 shows the fit indices of the measurement models.
The combined reliability coefficient and Cronbach α coefficient are at a very favorable level and the AVE of the constructs is also favorable.
Divergent validity (fornell and larcker method)
Another vital criterion is divergent validity; divergent validity complements convergent validity, which is measured through the Fornell-Larker test (Table 4).
Structural model fit (relationships between latent variables)
Coefficient of determination index (R2) Endogenous Variables
The coefficient R2 indicates the effect of an exogenous variable on an endogenous variable, and three values of 0.19, 0.33 and 0.67 are considered the criteria for weak, medium and strong values of R2. The higher R2 is related to the endogenous structures of a model, the better the fit of the model (Table 5).
The determination coefficients show that more than 70% of the changes are related to the variable of anxiety and sleep disorder. More than 45% of the changes are associated with the variable of depression symptomsand explain it. The rest of the changes in these variables are related to physical health, social functioning and other factors and components not considered in the model and research.
Predictive correlation index Q2
The criterion Q2 (Stone-Geisser) determines the model’s predictive power in the dependent variables. According to their belief, the models with an acceptable structural fit should be able to predict the indicators related to the endogenous structures of the model. Value Q2>0 indicates the model has a predictive fit for a given endogenous construct. On the other hand, zero and lower values indicate the lack of predictive fit. It determines three values: 0.02, 0.15 and 0.35, as low, medium and strong predictive power.
According to the Table 6, the prediction value Q2 of the model regarding the mentioned variables has moderate and appropriate power.
Overall model fit (combination of measurement and structural models)
After evaluating the measurement and structural models, the overall model (the sum of the measurement and structural models) should also be examined. For this purpose, Tenenhaus et al. introduced the GOF index [22]. The Equation 2 calculates this index and three values of 0.01, 0.25 and 0.36 are considered weak, medium and strong. The closer the value of this person is to 1, the stronger the overall model.
As seen in the Table 7, the value of the GOF index of the model is equal to 0.310, which means that the model is relatively suitable.
Examining research hypotheses
Discussion
The results of this study showed that bullying in the workplace has significant negative effects on the mental health of employees. Based on the fact that the path coefficient in the first hypothesis is estimated at 0.809, with a significance level of 0.000 and a t=25.131, which is both <0.05 and >1.96, this path coefficient is significant at the 0.05 error level (Table 8).
Therefore, with 95% confidence, the first hypothesis of the study, which suggests that organizational bullying impacts anxiety and sleep disorders, is accepted. Nauman et al. (2019) demonstrated that workplace bullying leads to increased job-related anxiety and insomnia, which subsequently reduces employees’ life satisfaction. The findings of hypothesis 1 align with these results, as this study also shows that workplace and environmental threats stemming from bullying lead to job anxiety and poor sleep quality. These similarities, particularly regarding the psychological effects of bullying and its impact on employees’ mental health, reveal significant consistency with Nauman et al. research [14]. Similarly, Lo Presti et al. highlighted the association between workplace bullying and anxiety and depression, identifying these two variables as mediators in the relationship [13].
Consistent with this study, the findings of hypothesis 1 reveal that workplace bullying directly contributes to the onset of depression. Specifically, the significant relationship between bullying, depression and anxiety in this research mirrors the findings of Lo Presti et al. emphasizing the direct negative effects of bullying behaviors on employees’ mental health. The innovation of this research lies in its focus on the types of bullying threats and their specific effects on mental health. Notably, this hypothesis examines the impact of bullying in distinct areas, such as job-related threats, social threats, and physical health threats—dimensions that have received less attention in some prior studies. These findings, supported by up-to-date data and a broad sample population, provide a more comprehensive perspective on the effects of workplace bullying. This detailed analysis clarifies the relationships between bullying and specific psychological outcomes, such as anxiety and sleep disorders, with greater precision. It can be explained that bullying in the workplace has significant negative effects on employees’ mental health, especially in increasing the level of anxiety and sleep disorders. This relationship can be explained through various mechanisms such as increased stress, decreased sense of control over job tasks and additional cognitive load. In particular, the constant stress caused by bullying can lead to intrusive thoughts and nightly worries, which in turn lead to insomnia and increased anxiety. Based on the fact that the path coefficient in the second hypothesis is estimated to be 0.675 and considering the significance level of 0.000 and the significance value of 14.507, which are both <0.05 and >1.96, this path coefficient is significant at the 0.05 error level. Therefore, with 95% confidence, it can be stated that the second hypothesis of the research, which suggests that organizational bullying affects depression, is accepted. Török et al. in a study conducted on 2478 employees in Denmark, found that individuals exposed to bullying by their leaders experienced more severe symptoms of depression [16]. The findings of the second hypothesis in this study similarly indicate that organizational bullying can directly influence the severity of depression, aligning with the results of this research. Additionally, Rodell et al. emphasized in their study that bullying can significantly increase the level of depression and have long-term effects on employees’ mental health [17].
The results of this hypothesis also confirm this impact, showing a significant relationship between organizational bullying and depression. According to Nielsen and Einarsen, exposure to systematic and prolonged aggressive behaviors negatively impacts the individual, causing cognitive activation and subsequent physiological activation that, if prolonged, damage health and well-being. In particular, given that each subject can have different consequences and show different reactions, leading to changes in cognitive-emotional balance (such as depression, anxiety, obsessions, panic attacks, emotional numbness) as well as in psychosomatic balance (such as digestive disorders) [23]. Considering that the path coefficient in the fourth hypothesis is estimated to be 0.647 and the significance level is 0.000, with a significance value of 11.590, which is <0.05 and >1.96, it can be concluded that this path coefficient is significant at the 0.05 error level. Therefore, with 95% confidence, the fourth hypothesis of the research, which suggests that organizational bullying negatively affects social functioning, is accepted. The results of this hypothesis are consistent with the research of Einarsen and Raknes [24].
This study focuses on the impact of bullying on reducing social interactions and increasing social isolation in the workplace. The results show that bullying victims are less likely to engage in positive interactions with their colleagues and tend to avoid social activities in the workplace. Your research also shows a similar impact on social functioning but with a focus on more specific outcomes. The innovation of this study lies in the fact that, unlike previous studies, which mainly referenced the reduction of interactions or feelings of isolation, our research specifically examines the functional consequences resulting from the reduction of social interactions. In explaining this relationship, it is stated that workplace bullying has significant effects on employees’ negative social functioning. Victims of bullying often suffer from a decrease in self-confidence and social activities, which can lead to a decrease in positive interactions with colleagues and a decrease in cooperation in the workplace. Bullying behaviors not only weaken professional and social relationships but also affect employees’ sense of belonging and motivation. These conditions can decrease the overall productivity and efficiency of the organization. Therefore, creating supportive work environments, formulating effective policies to deal with bullying, and providing training and support programs to strengthen employees’ social skills can help to improve social functioning and promote their mental and professional health.
Conclusion
The results of this research emphasize the need to pay attention to employees’ mental health and to adopt preventive measures against bullying in the workplace. To reduce the negative impacts of organizational bullying, managers should implement practical and effective actions to support employees and improve working conditions. Therefore, with the results obtained from this research, managers should take practical and effective measures to reduce the adverse effects of organizational bullying on the mental health of Bojnourd Municipality employees. It is suggested that clear and specific anti-bullying policies be formulated and implemented and confidential reporting systems be designed to facilitate complaints. Also, holding training courses to increase the awareness and communication skills of employees and managers, creating a supportive work environment encouraging positive behaviors and providing counseling and psychological support to victims of bullying can help improve employees’ mental health and the quality of the work environment. These measures will generally prevent bullying and improve the quality of interactions and mental health in the workplace.
Study limitations
This study focuses solely on the employees of the Bojnourd Municipality. Therefore, the results may not be fully generalizable to other organizations or regions. Due to time limitations, this research has not examined the long-term effects of organizational bullying on employees’ mental health. It may only cover short-term or medium-term impacts. In this study, self-report methods (such as questionnaires and interviews) were used for data collection, and these methods are liable to challenges such as response bias or lack of honesty, which can affect the accuracy of the results.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Bojnourd Branch, Bojnourd, Iran (Code: IR.IAU.BOJNOURD.REC.1403.013).
Funding
The paper was extracted from the PhD thesis of Hosein Faraji, approved by Islamic Azad University of Bojnourd, Bojnourd, Iran.
Authors contributions
Conceptualization and supervision: Hamed Khorasani Toroghi and Vahid Mirzaei; Methodology: Hamed Khorasani Toroghi and Hossein Faraji; Data collection: Vahid Mirzaei and Hamed Khorasani Toroghi; Data analysis: Vahid Mirzaei and Hossein Faraji; Funding acquisition and resources: Hamed Khorasani Toroghi and Hossein Faraji; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the Student Research Committee of the Islamic Azad University of Bojnourd for supporting this research.
References
- Vijayakumar G, Rajagopal S. Workplace bullying among nurses: A systematic review. Multidisciplinary Reviews. 2024; 7:e2024019. [Link]
- Ramadhaniama DD, Sartika Y. Bullying portrayed by main character in Anne with an Eseries [PhD dissertation]. Surakarta: UIN Surakarta; 2023. [Link]
- Ariza-Montes A, Muniz NM, Montero-Simó MJ, Araque-Padilla RA. Workplace bullying among healthcare workers. International Journal of Environmental Research and Public Health. 2013; 10(8):3121-39. [DOI:10.3390/ijerph10083121] [PMID]
- Raypole C. How to identify and manage workplace bullying. Health line. 2019. [Link]
- RobertF. Impact of workplace bullying on job performance and job stress. Journal of Management Info. 2018; 5(3):12-5. [Link]
- Huang H, Yu S, Peng P. Can organizational identification weaken the negative effects of customer bullying?-Testing the moderating effect of organizational identification. Frontiers in Psychology. 2022; 13:769087. [DOI:10.3389/fpsyg.2022.769087] [PMID]
- Campbell M. Loneliness, social anxiety and bullying victimization in young people: A literature review. Psychology and Education. 2013; 50(3-4):1-10. [Link]
- Green C. The hollow: A theory on workplace bullying in nursing practice. NursingForum. 2021; 56(2):433-8. [DOI:10.1111/nuf.12539] [PMID]
- Nielsen MB, Nielsen GH, Notelaers G, Einarsen S. Workplace Bullying and Suicidal Ideation: A 3-Wave Longitudinal Norwegian Study. American Journal of Public Health. 2015; 105(11):e23-8. [PMID]
- Hui EK, Tsang SK, Law BC. Combating school bullying through developmental guidance for positive youth development and promoting harmonious school culture. The Scientific World Journal. 2011;11:2266-77. [DOI:10.1100/2011/705824] [PMID]
- Rosander M, Blomberg S. Levels of workplace bullying and escalation-a new conceptual model based on cut-off scores, frequency and self-labelled victimization. European Journal of Work and Organizational Psychology. 2019; 28(6):769-83. [DOI:10.1080/1359432X.2019.1642874]
- Reknes I, Pallesen S, Magerøy N, Moen BE, Bjorvatn B, Einarsen S. Exposure to bullying behaviors as a predictor of mental health problems among Norwegian nurses: Results from the prospective SUSSH-survey. International Journal of Nursing Studies. 2014; 51(3):479-87. [DOI:10.1016/j.ijnurstu.2013.06.017] [PMID]
- Lo Presti A, Pappone P, Landolfi A. The associations between workplace bullying and physical or psychological negative symptoms: Anxiety and depression as mediators. Europe's Journal of Psychology. 2019; 15(4):808-22. [DOI:10.5964/ejop.v15i4.1733] [PMID]
- Nauman S, Malik SZ, Jalil F. How Workplace Bullying Jeopardizes Employees' Life Satisfaction: The Roles of Job Anxiety and Insomnia. Frontiers in Psychology. 2019 ;10:2292. [DOI:10.3389/fpsyg.2019.02292] [PMID]
- Lee RT, Lovell BL, Brotheridge CM. Tenderness and steadiness: Relating job and interpersonal demands and resources with burnout and physical symptoms of stress in Canadian Physicians. Journal of Applied Social Psychology. 2010; 40(9):2319-42. [DOI:10.1111/j.1559-1816.2010.00658.x]
- Török E, Hansen ÅM, Grynderup MB, Garde AH, Høgh A, Nabe-Nielsen K. The association between workplace bullying and depressive symptoms: The role of the perpetrator. BMC Public Health. 2016; 16:993. [DOI:10.1186/s12889-016-3657-x] [PMID]
- Rodell JB, Judge TA. Can “good” stressors spark “bad” behaviors? The mediating role of emotions in links of challenge and hindrance stressors with citizenship and counterproductive behaviors. Journal of Applied Psychology. 2009; 94(6):1438-51. [PMID]
- Leymann H. The content and development of mobbing at work. European Journal of Work and Organizational Psychology. 1996; 5(2):165-84. [DOI:10.1080/13594329608414853]
- Şahin T. The relationship between mobbing and organizational commitment among nurses [MA thesis]. Turkey: Marmara Universitesi; 2012. [Link]
- Goldberg DP, Hillier VF. A scaled version of the General Health Questionnaire. Psychological Medicine. 1979; 9(1):139-45. [DOI:10.1017/S0033291700021644] [PMID]
- Holland CP, Light B, Gibson N. A critical success factors model for enterprise resource planning implementation. Paper presented at: 7th European Conference on Information Systems. 23-25 June, 1999; Brisbane, Australia. [Link]
- Tenenhaus M, Amato S, Esposito Vinzi V. A global goodness-of-fit index for PLS structural equation modelling. Proceedings of the XLII SIS Scientific Meeting. 2004 ; 1( 2):739-42. [Link]
- Nielsen MB, Einarsen S. Outcomes of exposure to workplace bullying: A meta-analytic review. Work & Stress. 2012; 26(4):309-32. [DOI:10.1080/02678373.2012.734709]
- Einarsen S, Raknes BI. Harassment in the workplace and the victimization of men. Violence and Victims. 1997; 12(3):247-63. [DOI:10.1891/0886-6708.12.3.247] [PMID]
Type of Study: Original Article |
Subject:
Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
