

Volume 11, Issue 4 (Autumn 2023)
Iran J Health Sci 2023, 11(4): 259-270 |
Back to browse issues page


Ethics code: IR.SSU.REC.1400.033
Clinical trials code: none
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rashidi Maybodi F, Zeighami A, Toodehzaeim M H. Knowledge, Attitude, and Practice of Oral Healthcare Among Patients With Fixed Orthodontic Appliance: A Cross-sectional Survey in Yazd City, Iran. Iran J Health Sci 2023; 11 (4) :259-270
URL: http://jhs.mazums.ac.ir/article-1-890-en.html
URL: http://jhs.mazums.ac.ir/article-1-890-en.html



Department of Periodontics, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. , f_rashidi63@yahoo.com
Full-Text [PDF 851 kb]
(132 Downloads)
| Abstract (HTML) (591 Views)
Full-Text: (80 Views)
1. Introduction
Orthodontic treatment improves the occlusal relationship. It helps with better chewing, speech, aesthetics, and oral health [1]. In other words, improper occlusal relationship and irregularity of teeth, such as crowding, are predisposing factors for plaque accumulation. So, the orthodontic treatment directly corrects any dental and facial abnormalities and indirectly improves the health of the periodontium [2].
However, orthodontic treatment may also cause complications [1]. Oral healthcare becomes difficult due to brackets and wires [3, 4]. Self-cleansing also becomes difficult due to the low mechanical chewing and rinsing effect of saliva on food residues [5]. Therefore, biofilm accumulation may gradually lead to white spots, caries, periodontal disease, and halitosis [6-11].
Therefore, patients should be aware that failure to comply with the oral hygiene protocol leads to the termination of treatment [12]. Also, patients should know the correct method of brushing and using an interdental toothbrush and mouthwash, and these behaviors should be promoted during the treatment [13]. Patients must clearly acknowledge the significance of follow-up sessions [2, 5]. Follow-up must include periodontal probing every 6 months, so if a pathological pocket is found, further radiographic examination or referral to a periodontist can be done to restore oral health [14].
Ilyas’s study in Pakistan shows that most patients are aware of oral hygiene practices during orthodontic treatment and perform them, but not at desirable levels [6]. A study by Ajayi et al. shows that most orthodontic patients (62.8%) exhibit good oral hygiene, which increases the likelihood of optimal orthodontic results [8]. Since there was little information about the knowledge, attitude, and practice of patients with fixed appliances referred to the orthodontic Department of Yazd Dental School, Yazd City, Iran, regarding oral health, this study was designated and implemented to fill this gap.
2. Materials and Methods
Study design
This research is a descriptive-analytical study conducted at the Orthodontics Department of the School of Dentistry, Yazd University of Medical Sciences, between August 2021 and March 2022. The inclusion criterion was the consent of patients under fixed orthodontics treatment to participate in the study. The exclusion criterion included an incomplete questionnaire.
Sample size and sampling method
Considering the of 95% Cl and according to a previous similar article regarding the status of knowledge of 25% (P), α= 5% and the estimation error of 6% (E) [15], the sample size was estimated as 201. They were recruited by convenience sampling (Equation 1):

Study tool
A questionnaire in four parts was developed for this study. The first part included the participants’ demographic data (age, gender, education level, and treatment duration). The second part aimed to assess the participants’ knowledge by 7 questions. The third part contained 7 questions evaluating participants’ attitudes regarding oral health. The fourth part consisted of 8 questions about oral health practice. All patients were asked to complete the questionnaire in the waiting room in the Orthodontic Department and return it within 20 minutes.
Validity and reliability assessment
The Lawshe model was used to determine the content validity of the questionnaire. Three criteria, including necessity, transparency and relevance were examined to check the content validity. The questionnaire was reviewed by a panel of experts in the Dental Faculty of Dentistry, consisting of 6 periodontists, 2 orthodontists, and 1 faculty member from the Department of Oral Health and Community Dentistry. The opinions of the 10 panelists were determined by the content validity ratio (CVR) of 0.75. If the CVR value were less than 0.7, the item would be rejected, and accordingly, no item was excluded. The questionnaire was distributed 20 days before conducting the study to 25 patients drawn from the same sampling frame to evaluate the questions’ applicability, ease of understanding, and clarity. No major amendments were required following feedback from the pilot. The Cronbach α was calculated as 0.74, which is good for the reliability of a new questionnaire.
The data were collected by completing the questionnaire via the self-administered method by the participants. Still, in case of problems in understanding some questions, the interviewer gave explanations.
Data analysis
For the knowledge questions, 1 point was given for the correct answer to the knowledge questions, 0.5 points for “I don’t know,” and 0 points for the wrong answer. The following classification was considered to report the patients’ knowledge level qualitatively: Score 6-7 as good, score 4-6 as moderate, score 3-4 as poor, and 3 or less as very poor. In the practice part, a score of 6-8 was considered good, 6-4 as average, 3-4 as poor, and 3 or less as very poor.
Answers to the attitude questions were reported by their frequency and were not scored. The answers only showed the patient’s attitude and did not necessarily have a correct answer.
The data were analyzed with the t-test, analysis of variance (ANOVA), and chi-square using SPSS software, version 25. The level of significance in this study was considered <0.05.
3. Results
Of 201 patients asked to complete the questionnaire, 199 responded, and 2 submitted incomplete questionnaires and were replaced by two new participants.
Demographic baseline data
The Mean±SD age of participants was 19.65±6.03 years within the range of 10-37 years. The participants were 70(36.8%) men and 127(63.2%) women. The demographic information of the patients is shown in Table 1.

Knowledge about oral health
The Mean±SD score of knowledge, which could be from 0 to 7, was obtained as 5±1.13, considered moderate. There was no significant association between knowledge and gender, age, treatment duration, and educational level (Table 2).

The frequency distribution of answers to knowledge questions is mentioned in Table 3. No correlation with demographic characteristics was also seen in the separate question-by-question evaluation, although these findings were not reported in detail to summarize the results.

Attitudes about oral health
As described in the study method, the overall mean score was not calculated in the attitude part due to lacking a specific correct answer for these questions, and the association between the mean score and demographic factors was not reported.
The frequency distribution of answers to these questions is shown in Table 3. Demographic variables had no significant effect on the frequency of responses to attitudinal questions, except for a few items mentioned below.
In this section, the gender variable made a significant difference only in questions 6 and 7, so in the sixth question, the “yes” answer was more among the males, and in the seventh question, the “yes” answer was more among the females. The two variables of age and duration of treatment did not make a significant difference in any question. The level of education made a significant difference only in the fifth question, so the higher the level of education, the higher the frequency of “yes” answers (Table 4).

Practice on oral health
The Mean±SD score of practice, which could range from 0 to 8, was obtained as 3.92±1.43, which was considered “poor” and was not statistically associated with demographic variables in general (Table 2). In a separate question-by-question review, gender and age variables did not make a significant difference in any question. The treatment duration variable significantly differed only in questions 4 and 5. In these two questions, with an increase in treatment duration, both the use of regular dental floss and special orthodontic floss were reduced (Table 4). The frequency distribution of answers to practice questions is shown in Table 4.
4. Discussion
Without adequate oral hygiene, the positive effects of orthodontic treatment may be lost [16]. Therefore, before starting the treatment, the dentist must ensure the patient can follow the oral hygiene instructions sufficiently. If the patient does not follow the necessary oral hygiene tips during the treatment, the active orthodontic treatment should be postponed until the plaque control is improved [12]. So, patients should be aware of the importance of proper oral hygiene before and during orthodontic treatment. In the present study, knowledge about oral health among patients undergoing fixed orthodontic treatment was evaluated at a “moderate” level, and their practice was assessed at a “poor” level.
Unlike the study of Eid [17], Shah [18], and Priyadarsi [19], in which most participants were male, in this study, 63.2% of the participants were female, which is similar to the selected population of the studies of Sawai [20], Petrauskiene [21], Sharma [22], and Aljohani [23] in which the majority of patients were female. The possible reason is that women are more concerned about esthetics and are more often referred for orthodontic treatment [24]. Since questionnaires were distributed in the follow-up appointments, it seems that women showed more regular presence in recalls. The Mean± SD age of the patients was 19.65±6.03 years. This young population can be attributed to the dentist’s suggestion to start treatment or the fact that young people are more willing to have a more beautiful appearance to gain more social acceptance.
In this study, the knowledge score was considered an average level, consistent with Priyadarsi’s study [19]. Unlike some previous studies in which the level of knowledge of females was higher than that of males [25-30], in our research, the knowledge score had no significant association with gender, which was consistent with Al-harbi [15] and Priyadarsi [19] studies. Unlike the study of Alhaija [25] and Al-harbi [15], the knowledge score in the present study had no significant association with the education level of the patients. In the study of Aikins [28], knowledge was higher in adolescents and those treated for more than 18 months. However, in this study, knowledge was not affected by age or duration of treatment. Likewise, the study of Alhaija [25] and Al-harbi [15] showed no difference in patients’ knowledge levels based on age. In some studies, such as Buthelezi [31], there was no mention of how knowledge is related to the age or gender of the participants.
It should be noted that similar studies comparing patients’ attitudes toward orthodontic treatment are very limited and mainly focused on knowledge and practice. In our study, as in similar articles, the main reason for orthodontic treatment was aesthetic [32, 33]. In our study, most participants believed improving oral hygiene could enhance social relationships. About 63.2% of the patients thought that orthodontic treatment is prohibited in adulthood, and 73.6% considered it necessary to ensure the health of the gums before starting orthodontic treatment. Interestingly, 87.5% of the participants had no opinion on whether orthodontic treatment should be postponed until after child delivery, or they mistakenly believed that pregnancy is an obstacle to starting this non-invasive treatment. In the present study, most people (89%) had met their dentist regularly after placing fixed orthodontic appliances. Also, they agreed with the need to increase brushing frequency during orthodontic treatment. In some studies, a majority of orthodontic patients (>90%) brushed their teeth at least twice a day [2, 15, 25]. In our study, only 61.7% of the patients brushed their teeth twice a day or more, which shows a lack of adherence to regular brushing, consistent with some previous studies [17, 18, 20, 34, 35]. Insufficient brushing during orthodontic treatment leads to plaque accumulation around the brackets. Therefore, the dentist should again emphasize the value of brushing during every visit.
Of course, it should be noted that increasing the frequency of brushing alone is not enough because brushing technique is a more important key factor in maintaining oral health [36, 37]. In the present study, similar to the study of Pandey [35], the main brushing technique used by the participants was a combination of horizontal and vertical movements. Toothbrushes with hard bristles remove more dental plaques but cause more abrasion on the gingiva and tooth surface. Therefore, a hard toothbrush is not recommended by healthcare professionals. Fortunately, our findings showed that only 4.5% of patients used a hard toothbrush, similar to the study by Atassi et al. in Saudi Arabia [34]. In Pandey’s study, about one-fifth of patients used brushes with hard bristles; interestingly, more than half never noticed the toothbrush they were using [35].
In our study, most participants (68.2%) used a medium toothbrush, while in Lee [36] and Guo [38], most participants used soft ones. An orthodontic toothbrush is a two-surface toothbrush with longer bristles on the edges and shorter bristles in the middle. This brush cleans the brackets’ top and bottom [39]. In our study, more than half of the people used a special orthodontic toothbrush, which is consistent with the investigations of Atanasova [40] and Anuwongnukroh [39]. In our study, compared to Guo’s study [38], patients changed their toothbrushes after a longer period, which may be due to the economic conditions or lack of knowledge about toothbrush’s effectiveness decrease over time.
Daily use of mouthwashes containing fluoride will significantly reduce white spots around bands and brackets and minimize the occurrence of enamel demineralization during treatment [41]. In our study, like some previous studies [36, 39], more than half of the people used fluoride mouthwash, which could be due to the installation of an educational poster on the wall of the Orthodontic Department about the effect of fluoride mouthwash in preventing caries or due to the impact of health instructions given to the patients by post-graduates. This finding was unlike the studies of Guo [38] and Khraisat [42], where a minority of patients used mouthwash.
Dental floss helps remove plaque from the interdental spaces [40, 43]. However, flossing under wires and brackets is challenging, and the patients’ cooperation may decrease [39]. Nevertheless, in our study, most people used dental floss, which was inconsistent with some previous studies [35, 38, 40, 44]. However, our study reported the frequency of super-floss usage in only about 1 out of 4 patients. In this study, most patients believed oral healthcare during orthodontic treatment should be more than usual. Still, this positive attitude did not necessarily lead to positive practice. In our study, as in Čalušić’s study [44], for most people (58.7%), the fixed orthodontic appliance did not cause any problems in oral hygiene compared to the past. Unfortunately, unlike the study of Ilyas [6], in which 78% of people had their teeth scaled during orthodontic treatment, in our study, only one out of four patients had scaling during their treatment.
In practice questions, with the increase in treatment duration, patients’ cooperation in using regular dental floss as well as special orthodontic dental floss decreased, which may be due to patients’ tiredness of following hygiene principles, reducing their internal motivation, or reducing the effectiveness of oral hygiene instructions taught at the beginning of treatment.
The difference in the results in various studies may be due to the diversity in culture, the developmental status of the country of the study, or perhaps demographic characteristics, such as the socioeconomic status, the level of education, and the type of health instructions received from the dentist.
5. Conclusion
Knowledge of oral health among patients undergoing fixed orthodontic treatment was evaluated as “moderate” and their practice as “poor.” There are some negative attitudes towards orthodontic treatment, such as an unsafe treatment in pregnancy or the impossibility of orthodontic treatment in adulthood, which should be rectified. Educational interventions are suggested due to the need to improve patients’ knowledge, attitude, and practice about oral hygiene during orthodontic treatment.
Study limitations
The results of this study could not be generalized to the entire urban society due to the similar socioeconomic class of patients referred to the Dental School. It can be helpful to compare our findings with the results of future patients referred to the private treatment sector.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Sadoughi University of Medical Sciences (Code: IR.SSU.REC.1400.033), and written informed consent was obtained from all participants.
Funding
This research was derived from thesis NO. 14040 supported by Shahid Sadoughi University of Medical Sciences.
Authors contributions
Conceptualizations, study design and conduct the study: Ayda Zeighami; Analysis, data interpretation, Writing the manuscript: Fahimeh Rashidi Maybodi; Preparing the questionnaire and sampling: Mohammad Hossein Toodehzaeim; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors are grateful to all the patients who participated in this study.
References
Orthodontic treatment improves the occlusal relationship. It helps with better chewing, speech, aesthetics, and oral health [1]. In other words, improper occlusal relationship and irregularity of teeth, such as crowding, are predisposing factors for plaque accumulation. So, the orthodontic treatment directly corrects any dental and facial abnormalities and indirectly improves the health of the periodontium [2].
However, orthodontic treatment may also cause complications [1]. Oral healthcare becomes difficult due to brackets and wires [3, 4]. Self-cleansing also becomes difficult due to the low mechanical chewing and rinsing effect of saliva on food residues [5]. Therefore, biofilm accumulation may gradually lead to white spots, caries, periodontal disease, and halitosis [6-11].
Therefore, patients should be aware that failure to comply with the oral hygiene protocol leads to the termination of treatment [12]. Also, patients should know the correct method of brushing and using an interdental toothbrush and mouthwash, and these behaviors should be promoted during the treatment [13]. Patients must clearly acknowledge the significance of follow-up sessions [2, 5]. Follow-up must include periodontal probing every 6 months, so if a pathological pocket is found, further radiographic examination or referral to a periodontist can be done to restore oral health [14].
Ilyas’s study in Pakistan shows that most patients are aware of oral hygiene practices during orthodontic treatment and perform them, but not at desirable levels [6]. A study by Ajayi et al. shows that most orthodontic patients (62.8%) exhibit good oral hygiene, which increases the likelihood of optimal orthodontic results [8]. Since there was little information about the knowledge, attitude, and practice of patients with fixed appliances referred to the orthodontic Department of Yazd Dental School, Yazd City, Iran, regarding oral health, this study was designated and implemented to fill this gap.
2. Materials and Methods
Study design
This research is a descriptive-analytical study conducted at the Orthodontics Department of the School of Dentistry, Yazd University of Medical Sciences, between August 2021 and March 2022. The inclusion criterion was the consent of patients under fixed orthodontics treatment to participate in the study. The exclusion criterion included an incomplete questionnaire.
Sample size and sampling method
Considering the of 95% Cl and according to a previous similar article regarding the status of knowledge of 25% (P), α= 5% and the estimation error of 6% (E) [15], the sample size was estimated as 201. They were recruited by convenience sampling (Equation 1):
Study tool
A questionnaire in four parts was developed for this study. The first part included the participants’ demographic data (age, gender, education level, and treatment duration). The second part aimed to assess the participants’ knowledge by 7 questions. The third part contained 7 questions evaluating participants’ attitudes regarding oral health. The fourth part consisted of 8 questions about oral health practice. All patients were asked to complete the questionnaire in the waiting room in the Orthodontic Department and return it within 20 minutes.
Validity and reliability assessment
The Lawshe model was used to determine the content validity of the questionnaire. Three criteria, including necessity, transparency and relevance were examined to check the content validity. The questionnaire was reviewed by a panel of experts in the Dental Faculty of Dentistry, consisting of 6 periodontists, 2 orthodontists, and 1 faculty member from the Department of Oral Health and Community Dentistry. The opinions of the 10 panelists were determined by the content validity ratio (CVR) of 0.75. If the CVR value were less than 0.7, the item would be rejected, and accordingly, no item was excluded. The questionnaire was distributed 20 days before conducting the study to 25 patients drawn from the same sampling frame to evaluate the questions’ applicability, ease of understanding, and clarity. No major amendments were required following feedback from the pilot. The Cronbach α was calculated as 0.74, which is good for the reliability of a new questionnaire.
The data were collected by completing the questionnaire via the self-administered method by the participants. Still, in case of problems in understanding some questions, the interviewer gave explanations.
Data analysis
For the knowledge questions, 1 point was given for the correct answer to the knowledge questions, 0.5 points for “I don’t know,” and 0 points for the wrong answer. The following classification was considered to report the patients’ knowledge level qualitatively: Score 6-7 as good, score 4-6 as moderate, score 3-4 as poor, and 3 or less as very poor. In the practice part, a score of 6-8 was considered good, 6-4 as average, 3-4 as poor, and 3 or less as very poor.
Answers to the attitude questions were reported by their frequency and were not scored. The answers only showed the patient’s attitude and did not necessarily have a correct answer.
The data were analyzed with the t-test, analysis of variance (ANOVA), and chi-square using SPSS software, version 25. The level of significance in this study was considered <0.05.
3. Results
Of 201 patients asked to complete the questionnaire, 199 responded, and 2 submitted incomplete questionnaires and were replaced by two new participants.
Demographic baseline data
The Mean±SD age of participants was 19.65±6.03 years within the range of 10-37 years. The participants were 70(36.8%) men and 127(63.2%) women. The demographic information of the patients is shown in Table 1.
Knowledge about oral health
The Mean±SD score of knowledge, which could be from 0 to 7, was obtained as 5±1.13, considered moderate. There was no significant association between knowledge and gender, age, treatment duration, and educational level (Table 2).
The frequency distribution of answers to knowledge questions is mentioned in Table 3. No correlation with demographic characteristics was also seen in the separate question-by-question evaluation, although these findings were not reported in detail to summarize the results.
Attitudes about oral health
As described in the study method, the overall mean score was not calculated in the attitude part due to lacking a specific correct answer for these questions, and the association between the mean score and demographic factors was not reported.
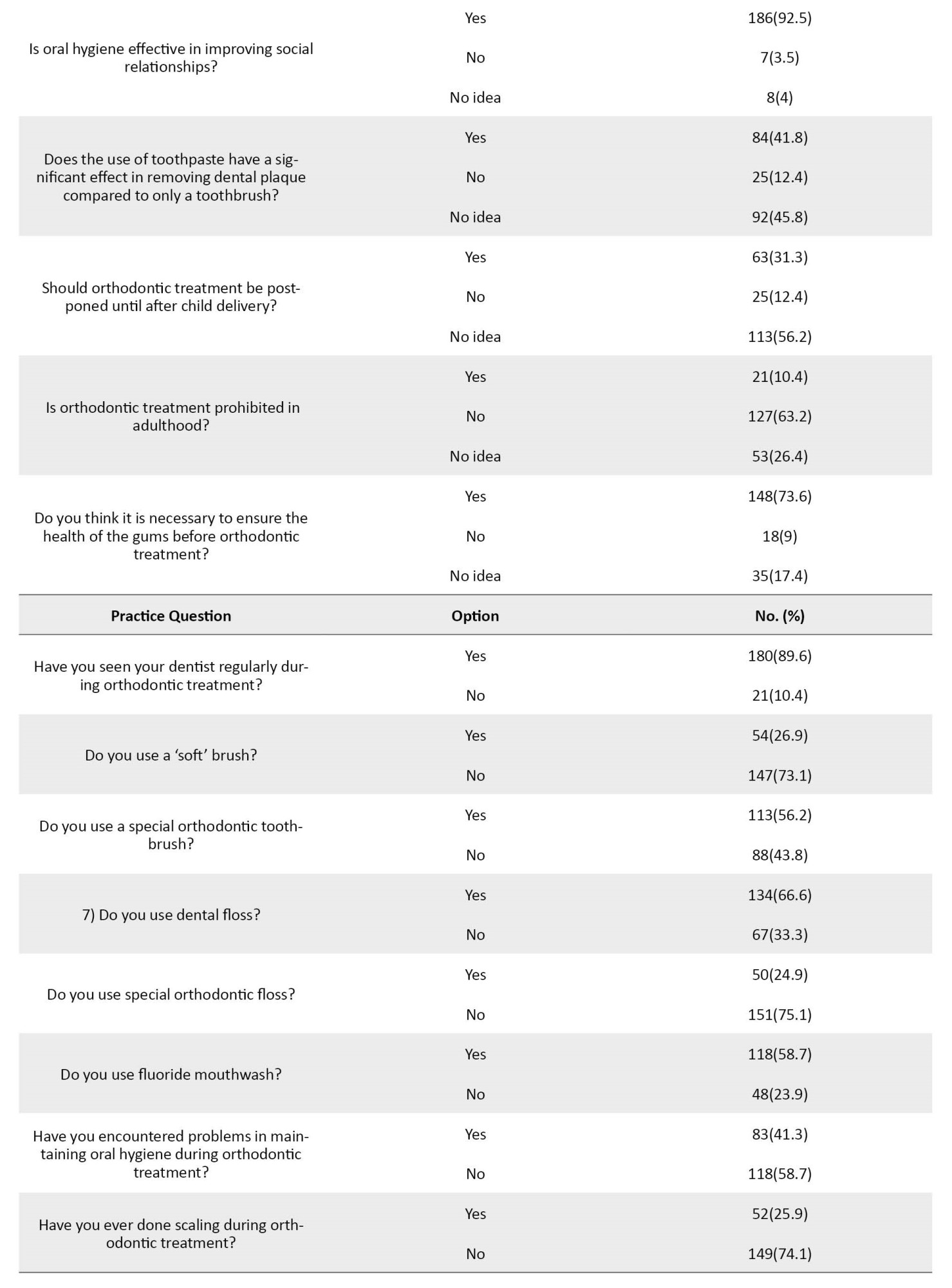
The frequency distribution of answers to these questions is shown in Table 3. Demographic variables had no significant effect on the frequency of responses to attitudinal questions, except for a few items mentioned below.
In this section, the gender variable made a significant difference only in questions 6 and 7, so in the sixth question, the “yes” answer was more among the males, and in the seventh question, the “yes” answer was more among the females. The two variables of age and duration of treatment did not make a significant difference in any question. The level of education made a significant difference only in the fifth question, so the higher the level of education, the higher the frequency of “yes” answers (Table 4).
Practice on oral health
The Mean±SD score of practice, which could range from 0 to 8, was obtained as 3.92±1.43, which was considered “poor” and was not statistically associated with demographic variables in general (Table 2). In a separate question-by-question review, gender and age variables did not make a significant difference in any question. The treatment duration variable significantly differed only in questions 4 and 5. In these two questions, with an increase in treatment duration, both the use of regular dental floss and special orthodontic floss were reduced (Table 4). The frequency distribution of answers to practice questions is shown in Table 4.
4. Discussion
Without adequate oral hygiene, the positive effects of orthodontic treatment may be lost [16]. Therefore, before starting the treatment, the dentist must ensure the patient can follow the oral hygiene instructions sufficiently. If the patient does not follow the necessary oral hygiene tips during the treatment, the active orthodontic treatment should be postponed until the plaque control is improved [12]. So, patients should be aware of the importance of proper oral hygiene before and during orthodontic treatment. In the present study, knowledge about oral health among patients undergoing fixed orthodontic treatment was evaluated at a “moderate” level, and their practice was assessed at a “poor” level.
Unlike the study of Eid [17], Shah [18], and Priyadarsi [19], in which most participants were male, in this study, 63.2% of the participants were female, which is similar to the selected population of the studies of Sawai [20], Petrauskiene [21], Sharma [22], and Aljohani [23] in which the majority of patients were female. The possible reason is that women are more concerned about esthetics and are more often referred for orthodontic treatment [24]. Since questionnaires were distributed in the follow-up appointments, it seems that women showed more regular presence in recalls. The Mean± SD age of the patients was 19.65±6.03 years. This young population can be attributed to the dentist’s suggestion to start treatment or the fact that young people are more willing to have a more beautiful appearance to gain more social acceptance.
In this study, the knowledge score was considered an average level, consistent with Priyadarsi’s study [19]. Unlike some previous studies in which the level of knowledge of females was higher than that of males [25-30], in our research, the knowledge score had no significant association with gender, which was consistent with Al-harbi [15] and Priyadarsi [19] studies. Unlike the study of Alhaija [25] and Al-harbi [15], the knowledge score in the present study had no significant association with the education level of the patients. In the study of Aikins [28], knowledge was higher in adolescents and those treated for more than 18 months. However, in this study, knowledge was not affected by age or duration of treatment. Likewise, the study of Alhaija [25] and Al-harbi [15] showed no difference in patients’ knowledge levels based on age. In some studies, such as Buthelezi [31], there was no mention of how knowledge is related to the age or gender of the participants.
It should be noted that similar studies comparing patients’ attitudes toward orthodontic treatment are very limited and mainly focused on knowledge and practice. In our study, as in similar articles, the main reason for orthodontic treatment was aesthetic [32, 33]. In our study, most participants believed improving oral hygiene could enhance social relationships. About 63.2% of the patients thought that orthodontic treatment is prohibited in adulthood, and 73.6% considered it necessary to ensure the health of the gums before starting orthodontic treatment. Interestingly, 87.5% of the participants had no opinion on whether orthodontic treatment should be postponed until after child delivery, or they mistakenly believed that pregnancy is an obstacle to starting this non-invasive treatment. In the present study, most people (89%) had met their dentist regularly after placing fixed orthodontic appliances. Also, they agreed with the need to increase brushing frequency during orthodontic treatment. In some studies, a majority of orthodontic patients (>90%) brushed their teeth at least twice a day [2, 15, 25]. In our study, only 61.7% of the patients brushed their teeth twice a day or more, which shows a lack of adherence to regular brushing, consistent with some previous studies [17, 18, 20, 34, 35]. Insufficient brushing during orthodontic treatment leads to plaque accumulation around the brackets. Therefore, the dentist should again emphasize the value of brushing during every visit.
Of course, it should be noted that increasing the frequency of brushing alone is not enough because brushing technique is a more important key factor in maintaining oral health [36, 37]. In the present study, similar to the study of Pandey [35], the main brushing technique used by the participants was a combination of horizontal and vertical movements. Toothbrushes with hard bristles remove more dental plaques but cause more abrasion on the gingiva and tooth surface. Therefore, a hard toothbrush is not recommended by healthcare professionals. Fortunately, our findings showed that only 4.5% of patients used a hard toothbrush, similar to the study by Atassi et al. in Saudi Arabia [34]. In Pandey’s study, about one-fifth of patients used brushes with hard bristles; interestingly, more than half never noticed the toothbrush they were using [35].
In our study, most participants (68.2%) used a medium toothbrush, while in Lee [36] and Guo [38], most participants used soft ones. An orthodontic toothbrush is a two-surface toothbrush with longer bristles on the edges and shorter bristles in the middle. This brush cleans the brackets’ top and bottom [39]. In our study, more than half of the people used a special orthodontic toothbrush, which is consistent with the investigations of Atanasova [40] and Anuwongnukroh [39]. In our study, compared to Guo’s study [38], patients changed their toothbrushes after a longer period, which may be due to the economic conditions or lack of knowledge about toothbrush’s effectiveness decrease over time.
Daily use of mouthwashes containing fluoride will significantly reduce white spots around bands and brackets and minimize the occurrence of enamel demineralization during treatment [41]. In our study, like some previous studies [36, 39], more than half of the people used fluoride mouthwash, which could be due to the installation of an educational poster on the wall of the Orthodontic Department about the effect of fluoride mouthwash in preventing caries or due to the impact of health instructions given to the patients by post-graduates. This finding was unlike the studies of Guo [38] and Khraisat [42], where a minority of patients used mouthwash.
Dental floss helps remove plaque from the interdental spaces [40, 43]. However, flossing under wires and brackets is challenging, and the patients’ cooperation may decrease [39]. Nevertheless, in our study, most people used dental floss, which was inconsistent with some previous studies [35, 38, 40, 44]. However, our study reported the frequency of super-floss usage in only about 1 out of 4 patients. In this study, most patients believed oral healthcare during orthodontic treatment should be more than usual. Still, this positive attitude did not necessarily lead to positive practice. In our study, as in Čalušić’s study [44], for most people (58.7%), the fixed orthodontic appliance did not cause any problems in oral hygiene compared to the past. Unfortunately, unlike the study of Ilyas [6], in which 78% of people had their teeth scaled during orthodontic treatment, in our study, only one out of four patients had scaling during their treatment.
In practice questions, with the increase in treatment duration, patients’ cooperation in using regular dental floss as well as special orthodontic dental floss decreased, which may be due to patients’ tiredness of following hygiene principles, reducing their internal motivation, or reducing the effectiveness of oral hygiene instructions taught at the beginning of treatment.
The difference in the results in various studies may be due to the diversity in culture, the developmental status of the country of the study, or perhaps demographic characteristics, such as the socioeconomic status, the level of education, and the type of health instructions received from the dentist.
5. Conclusion
Knowledge of oral health among patients undergoing fixed orthodontic treatment was evaluated as “moderate” and their practice as “poor.” There are some negative attitudes towards orthodontic treatment, such as an unsafe treatment in pregnancy or the impossibility of orthodontic treatment in adulthood, which should be rectified. Educational interventions are suggested due to the need to improve patients’ knowledge, attitude, and practice about oral hygiene during orthodontic treatment.
Study limitations
The results of this study could not be generalized to the entire urban society due to the similar socioeconomic class of patients referred to the Dental School. It can be helpful to compare our findings with the results of future patients referred to the private treatment sector.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Sadoughi University of Medical Sciences (Code: IR.SSU.REC.1400.033), and written informed consent was obtained from all participants.
Funding
This research was derived from thesis NO. 14040 supported by Shahid Sadoughi University of Medical Sciences.
Authors contributions
Conceptualizations, study design and conduct the study: Ayda Zeighami; Analysis, data interpretation, Writing the manuscript: Fahimeh Rashidi Maybodi; Preparing the questionnaire and sampling: Mohammad Hossein Toodehzaeim; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors are grateful to all the patients who participated in this study.
References
- Preoteasa CT, Ionescu E, Preoteasa E. Risks and complications associated with orthodontic treatment. In: Bourzgui F, editor. Orthodontics. London: IntechOpen; 2012. [Link]
- Baheti M J, Toshniwal N G. Survey on oral hygiene protocols among orthodontic correction-seeking individuals. Journal of Education and Ethics in Dentistry. 2015; 5(1):8-13. [DOI:10.4103/0974-7761.178020]
- Marini I, Bortolotti F, Parenti SI, Gatto MR, Bonetti GA. Combined effects of repeated oral hygiene motivation and type of toothbrush on orthodontic patients: A blind randomized clinical trial. The Angle Orthodontist. 2014; 84(5):896-901. [DOI:10.2319/112113-856.1] [PMID]
- Madariaga ACP, Bucci R, Rongo R, Simeon V, D'Antò V, Valletta R. Impact of fixed orthodontic appliance and clear aligners on the periodontal health: A prospective clinical study. Dentistry Journal. 2020; 8(1):4. [DOI:10.3390/dj8010004] [PMID]
- Nadar S, Dinesh SS. A questionnaire study about oral hygiene awareness among orthodontic patients. International Journal of Orthodontic Rehabilitation. 2016; 7(3):97-100. [DOI:10.4103/2349-5243.192531]
- Ilyas M, Khalid MU, Qurat-Ul-Ain Arif S, Ashraf S. Oral hygiene awareness in orthodontic patients; A cross sectional survey. The Professional Medical Journal. 2019; 26(6):1000-4. [DOI:10.29309/TPMJ/2019.26.06.3574]
- Rao A, Hosadurga R, Vijaya K, Shankar RK, Boloor VA, Prathap S. Improvement in awareness levels and periodontal health among patients undergoing fixed orthodontic appliance therapy with established gingivitis and periodontal health maintenance program: A questionnaire based study. Journal of Oral Research. 2020; 9:500-10. [DOI:10.17126/joralres.2020.096]
- Ajayi EO, Azodo CC. Oral hygiene status among orthodontic patients attending university of Benin Teaching Hospital, Benin city, Nigeria. Journal of Dental Health, Oral Disorders & Therapy. 2014; 1(4):1-4. [DOI:10.15406/jdhodt.2014.01.00023]
- Höchli D, Hersberger-Zurfluh M, Papageorgiou SN, Eliades T. Interventions for orthodontically induced white spot lesions: A systematic review and meta-analysis. European Journal of Orthodontics. 2017; 39(2):122-33. [DOI:10.1093/ejo/cjw065] [PMID]
- Ghijselings E, Coucke W, Verdonck A, Teughels W, Quirynen M, Pauwels M, et al. Long-term changes in microbiology and clinical periodontal variables after completion of fixed orthodontic appliances. Orthodontics & Craniofacial Research. 2014; 17(1):49-59. [DOI:10.1111/ocr.12031] [PMID]
- Salvesen BF, Grytten J, Rongen G, Koldsland OC, Vandevska-Radunovic V. Periodontal status in long-term orthodontic retention patients up to 10 years after treatment - A cross-sectional study. Acta Odontologica Scandinavica. 2021; 79(8):623-9. [DOI:10.1080/00016357.2021.1921842] [PMID]
- Levin L, Einy S, Zigdon H, Aizenbud D, Machtei EE. Guidelines for periodontal care and follow-up during orthodontic treatment in adolescents and young adults. Journal of Applied Oral Science. 2012; 20(4):399-403. [DOI:10.1590/S1678-77572012000400002] [PMID]
- Avinash K, Gurumoorthy K. Knowledge of an orthodontist towards periodontal health care during orthodontic treatment. International Journal of Current Research. 2016; 8(11):41287-90. [Link]
- Moosa Y, Han LN, Safdar J, Sheikh OA, Pan YP. Periodontal status of Pakistani orthodontic patients. Brazilian Oral Research. 2015; 29:S1806-83242015000100285. [DOI:10.1590/1807-3107BOR-2015.vol29.0091] [PMID]
- Al-harbi AA, Alkhulayfi AS, Alharbi AT, Al-harbi M, Al-harbi AS, Al-harbi NS. Knowledge of patients about association between orthodontic treatment and periodontal diseases. International Journal of Oral Care and Research. 2018; 6(2):43-6. [Link]
- Matić S, Ivanović M, Mandić J, Nikolić P. [Possibilities to prevent gingivitis during fixed orthodontic appliance therapy (Croatian)]. Stomatološki glasnik Srbije. 2008; 55(2):122-32. [DOI:10.2298/SGS0802122M]
- Eid HA, Assiri HA, Kandyala R, Togoo RA, Turakhia VS. Gingival enlargement in different age groups during fixed Orthodontic treatment. Journal of International Oral Health. 2014; 6(1):1-4. [PMID] [PMCID]
- Shah K, Shenava S, Kulshrestha R, Hawaldar C. Evaluation of oral hygiene and perception of patients undergoing orthodontic treatment attending OPD at terna dental college, Mumbai, Maharashtra. International Dental Journal of Student's Research. 2018; 6(4):81-4. [DOI:10.18231/2278-3784.2018.0022]
- Priyadarsi U, Alam M, Hussain A, Azam F, Lal H, Parveen G. Awareness about periodontal health among patients with fixed orthodontic appliance. International Journal of Oral Care and Research. 2020; 8(2):20. [Link]
- Sawai DS, Singh P, Tushar, Dogra M, Sultana R, Khan SA. Perception, awareness, and practice among patients seeking orthodontic treatment toward maintenance of periodontal health and factors affecting the same among patients visiting dental clinics in Patna. Journal of Family Medicine and Primary Care. 2019; 8(11):3695-9. [DOI:10.4103/jfmpc.jfmpc_773_19] [PMID]
- Petrauskiene S, Wanczewska N, Slabsinskiene E, Zemgulyte G. Self-reported changes in oral hygiene habits among adolescents receiving orthodontic treatment. Dentistry Journal. 2019; 7(4):96. [DOI:10.3390/dj7040096] [PMID]
- Sharma JN. Pattern of distribution of malocclusions in patients seeking orthodontic treatment at BPKIHS from Sunsari District of Nepal. Health Renaissance. 2011; 8(2):93-6. [DOI:10.3126/hren.v8i2.4419]
- Aljohani SR, Alsaggaf DH. Adherence to dietary advice and oral hygiene practices among orthodontic patients. Patient Preference and Adherence. 2020; 14:1991-2000. [DOI:10.2147/PPA.S277034] [PMID]
- Isiekwe GI, Aikins EA. Self-perception of dental appearance and aesthetics in a student population. International Orthodontics. 2019; 17(3):506-12. [DOI:10.1016/j.ortho.2019.06.010] [PMID]
- Alhaija ESA, Al-Saif EM, Taani DQ. Periodontal health knowledge and awareness among subjects with fixed orthodontic appliance. Dental Press Journal of Orthodontics. 2018; 23(5):40.e1-40.e9. [DOI:10.1590/2177-6709.23.5.40.e1-9.onl] [PMID]
- Mathew R, Sathasivam HP, Mohamednor L, Yugaraj P. Knowledge, attitude and practice of patients towards orthodontic treatment. BMC Oral Health. 2023; 23(1):132.[DOI:10.1186/s12903-023-02780-y] [PMID] [PMCID]
- Shrestha RM, Bhattarai P, Dhakal J, Shrestha S. Knowledge, attitude and practice of patients towards orthodontic treatment: A multi-centric study. Orthodontic Journal of Nepal. 2014; 4(1):6-11. [DOI:10.3126/ojn.v4i1.11304]
- Aikins EA, Soroye MO. Periodontal status and oral hygiene compliance of orthodontic patients in a tertiary hospital in South-South Nigeria. International Journal of Dentistry and Oral Science. 2021; 8(10):4821-8. [Link]
- Wahengbam PP, Kshetrimayum N, Wahengbam BS, Nandkeoliar T, Lyngdoh D. Assessment of oral health knowledge, attitude and self-care practice among adolescents - a state wide cross- sectional study in Manipur, North Eastern India. Journal of Clinical and Diagnostic Research. 2016; 10(6):ZC65-70. [DOI:10.7860/JCDR/2016/20693.8002] [PMID] [PMCID]
- Kumar RP, Shrist N. Oral health knowledge, attitude, and practice of patients visiting a private hospital in Chennai. Journal of Dental Medicine. 2015; 14(6):12-5. [Link]
- Buthelezi NL, Madiba TK. Oral hygiene habits and status of orthodontic patients attending the University of Pretoria, Oral and Dental Hospital. South African Dental Journal. 2021 ; 76(3):130-5. [DOI:10.17159/2519-0105/2021/v76no3a2]
- Felemban OM, Alharabi NT, A Alamoudi RA, Alturki GA, Helal NM. Factors influencing the desire for orthodontic treatment among patients and parents in Saudi Arabia: A cross-sectional study. Journal of Orthodontic Science. 2022; 11:25. [DOI:10.4103/jos.jos_181_21] [PMID]
- Saccomanno S, Saran S, Laganà D, Mastrapasqua RF, Grippaudo C. Motivation, perception, and behavior of the adult orthodontic patient: A survey analysis. BioMed Research International. 2022; 2022:2754051. [DOI:10.1155/2022/2754051] [PMID]
- Atassi F, Awartani F. Oral hygiene status among orthodontic patients. The Journal of Contemporary Dental Practice. 2010; 11(4):25-32. [DOI:10.5005/jcdp-11-4-25]
- Pandey V, Chandra S, Dilip Kumar HP, Gupta A, Bhandari PP, Rathod P. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment: A cross-sectional study. Journal of International Society of Preventive & Community Dentistry. 2016; 6(2):120-4. [DOI:10.4103/2231-0762.178752] [PMID]
- Lee JH, Abdullah AAA, Yahya Na. Oral hygiene practices among fixed orthodontic patients in a university dental setting. International Journal of Oral Dental Health. 2016; 2(2):27. [DOI:10.23937/2469-5734/1510027]
- Berlin-Broner Y, Levin L, Ashkenazi M. Awareness of orthodontists regarding oral hygiene performance during active orthodontic treatment.European Journal of Paediatric Dentistry. 2012; 13(3):187-91. [PMID]
- Guo J, Li L, Guan G, Bennani F, Mei L. Oral health knowledge and practice among orthodontic clients in China and New Zealand. Canadian Journal of Dental Hygiene. 2020; 54(3):124-32. [PMID] [PMCID]
- Anuwongnukroh N, Dechkunakorn S, Kanpiputana R. Oral hygiene behavior during fixed orthodontic treatment. Dentistry. 2017; 7(10):1000457. [DOI:10.4172/2161-1122.1000457]
- Atanasova S, Carceva Salja S, Naskova S, Zarkova Atanasova J, Proseva L. Oral hygiene behavior during treatment with fixed orthodontic appliances. Journal of Dental and Medical Sciences. 2018; 17(11):67-71. [DOI:10.9790/0853-1711026771]
- Khoroushi M, Kachuie M. Prevention and treatment of white spot lesions in orthodontic patients. Contemporary Clinical Dentistry. 2017; 8(1):11-9. [DOI:10.4103/ccd.ccd_216_17] [PMID]
- Khraisat H M, Al-Shdeifat N A, Al-Alawneh A M, Al-Zyood A I, Al-Maani M O. Oral hygiene practices among fixed orthodontic patients in Az-zarqa, JordaN. Pakistan Oral & Dental Journal. 2016; 36(3):404. [Link]
- Zanatta FB, Moreira CH, Rösing CK. Association between dental floss use and gingival conditions in orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics. 2011; 140(6):812-21. [DOI:10.1016/j.ajodo.2011.06.028] [PMID]
- Čalušić Šarac M, Anić Milošević S, Matošić Ž, Lapter Varga M. Oral hygiene behavior of croatian adolescents during fixed orthodontic treatment: A cross-sectional study. Acta Stomatologica Croatica. 2021; 55(4):359-66. [DOI:10.15644/asc55/4/3] [PMID]
Type of Study: Original Article |
Subject:
Community Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
