

Volume 14, Issue 1 (Winter 2026)
Iran J Health Sci 2026, 14(1): 47-56 |
Back to browse issues page


Ethics code: IR.TABRIZU.REC.1404.023
Clinical trials code: 1944221
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esmaeilpour K, Khanjani Z, Ebrahimi varzaneh L. The Relationship Between Primary Emotional Traits and Adolescent Depression: The Mediating Role of Early Maladaptive Schemas. Iran J Health Sci 2026; 14 (1) :47-56
URL: http://jhs.mazums.ac.ir/article-1-1047-en.html
URL: http://jhs.mazums.ac.ir/article-1-1047-en.html



Department of Psychology, Faculty of Psychology and Educational Sciences, University of Tabriz, Tabriz, Iran. , leilaebrahimi2000@yahoo.com
Full-Text [PDF 1003 kb]
(286 Downloads)
| Abstract (HTML) (714 Views)
Full-Text: (177 Views)
Introduction
Adolescence is a critical developmental period marking the transition from childhood to adulthood and is characterized by emotional instability, evolving autonomy, and increased parent-child conflicts [1]. During this stage, adolescents develop more advanced cognitive abilities, including abstract thinking, explore their emerging sense of self and identity, and engage in comparisons regarding lifestyles and values as part of their psychosocial development [2]. Alongside these developmental changes, the risk of major depressive disorder (MDD) increases considerably, with depression typically emerging in mid-adolescence and often following a recurrent course [3]. Depressive symptoms during this period are linked to academic difficulties, impaired social functioning, substance use, and suicidal behaviors, with well-established risk factors such as family history, gender, maltreatment, chronic illness, emotional dispositions, and early maladaptive schemas (EMSs) [4].
Primary emotional traits—defined as evolutionarily rooted, biologically based affective tendencies such as sadness, fear, anger, seeking, and play—have been strongly associated with adolescent depression [4]. Empirical evidence indicates that heightened sadness, fear, and anger, accompanied by reduced seeking and play behaviors, significantly elevate depressive vulnerability. Among these, sadness appears to be the most strongly linked to depressive symptomatology [4]. Inadequate caregiving systems further diminish social engagement and emotional support, contributing to increased social isolation [5]. Neurobiological findings also suggest that fear- and distress-related processes are associated with reduced activation of reward circuitry, particularly during anticipation of positive social outcomes, thereby intensifying motivational deficits and negative affect [6]. Collectively, primary emotional traits may represent key vulnerability factors for depression by amplifying negative emotions, undermining motivation, and impairing social bonding [4].
EMSs are stable and pervasive cognitive-emotional patterns that often arise from adverse childhood experiences. These schemas significantly contribute to the emergence of depressive and anxiety symptoms during adolescence [7]. Rooted in Young schema theory, they can distort how individuals process information, intensify negative emotions, and are strongly linked to depression, anxiety, and difficulties in interpersonal relationships among adolescents and young adults [8]. The persistence of these schemas is reinforced through long-standing emotional-cognitive dysfunctions, which contribute to the stability of psychopathology across development [9].
Despite substantial evidence linking both primary emotional traits and EMSs to depressive symptoms, previous studies have not examined how these constructs interact within a unified framework. In particular, no study has evaluated whether EMSs mediate the relationship between primary emotional traits and adolescent depression, nor has research applied structural equation modeling (SEM) to test this mechanism during adolescence. This study investigates whether EMSs mediate the relationship between primary emotional traits and depressive symptoms in adolescents, addressing this critical gap in the existing literature.
Materials and Methods
This study employed a correlational design and targeted all male and female high school students (grades 10-12) aged 14–19 years living in Isfahan City, Iran. The minimum sample size was determined based on the recommended 1:15 ratio of participants to variables. Considering the 15 subscales of EMSs, 6 subscales of primary emotional traits, and the depression scale (a total of 22 subscales), a minimum of 330 participants was required.
A multistage cluster sampling method was used. First, permission was obtained from the Isfahan Department of Education. Then, 6 high schools (3 girls ‘and 3 boys’) were randomly selected from the city’s list of all public high schools. In the next stage, one class was randomly chosen from each selected school, and all students in those classes were invited to participate. The study objectives were explained to the students, and voluntary participation, confidentiality, and the right to withdraw at any time were emphasized. After excluding incomplete or invalid questionnaires, 253 students’ data remained and were included in the analyses.
The inclusion criteria consisted of being a high school student in grades 10–12, aged 14-19 years, and willingness to participate and complete the questionnaires. The exclusion criteria included incomplete questionnaires and withdrawal from participation at any stage.
Data analysis was performed using SPSS software, version 24 and AMOS software, version 24. SEM was used to examine the measurement and structural models. Model fit was evaluated using commonly recommended indices, including χ²/df, comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean square error approximation (RMSEA).
The following questionnaires were used to collect data.
Brief affective neuroscience personality scale (BANPS):
The BANPS assesses 6 primary emotional traits (seeking, care, play, anger, fear, and sadness) based on Panksepp’s affective neuroscience model. Responses are rated on a 5-point Likert scale. In previous research, the subscales demonstrated Cronbach α values ranging from 0.73 to 0.81 [10]. In the present study, the Cronbach α was 0.59 for positive emotional traits (seeking, care, play), 0.65 for negative traits (anger, fear, sadness), and 0.61 for the total scale, indicating relatively low internal consistency, which should be considered a limitation.
Composite scores for positive and negative emotional traits were based on theoretical considerations: seeking, care, and play were combined as positive traits, reflecting approach-related and affiliative emotional systems, while anger, fear, and sadness were combined as negative traits, reflecting avoidance-related and distress emotional systems [5].
Young schema questionnaire (YSQ)– short form (2003):
The YSQ is a 75-item instrument, rated on a 6-point Likert scale, that assesses 15 EMSs across five domains. The YSQ-SF has been extensively used in both clinical and research contexts and has demonstrated excellent reliability and validity in recent psychometric studies [11]. In the present study, the Cronbach α was 0.9 for the disconnection and rejection domain, 0.86 for impaired autonomy and performance, 0.78 for impaired limits, 0.80 for other-directedness, and 0.79 for hypervigilance and inhibition, with an overall reliability of 0.95 across all schemas.
In this study, EMSs were further categorized as follows: fundamental schemas, comprising the domains of disconnection and rejection, impaired autonomy and performance, and impaired limits; and compensatory schemas, comprising the domains of other-directedness and hypervigilance and inhibition. Scores for each domain were obtained from participants’ responses on the YSQ-SF.
Beck depression inventory-II (BDI-II)
The BDI-II is a 21-item multiple-choice instrument. It is designed to assess the severity of depressive symptoms, with scores ranging from 0 to 63, classified into 4 levels from minimal to severe. The BDI‑II is widely used in both research and clinical practice and demonstrates excellent psychometric properties, including high internal consistency (α≈0.9) and adequate test re-test reliability. Recent studies have confirmed that this tool exhibits strong validity and reliability, making it suitable for assessing depression across diverse populations [12]. In the current study, the Cronbach α was 0.9.
In this study, adolescent depression was defined as the total score obtained by participants on the BDI-II.
Results
A total of 253 individuals participated in this study. During the data screening process (to ensure multivariate normality), 2 participants were excluded. Thus, the final sample consisted of 251 participants. Among them, 195 participants (77.7%) were female, and 56(22.3%) were male. The mean and standard deviation of participants’ age were as follows: for girls, 16.42±0.83 years; for boys, 16.25±1.16 years; and for the total sample, 16.38±0.91 years. Table 1 presents the Mean±SD, skewness, and kurtosis for the study variables.
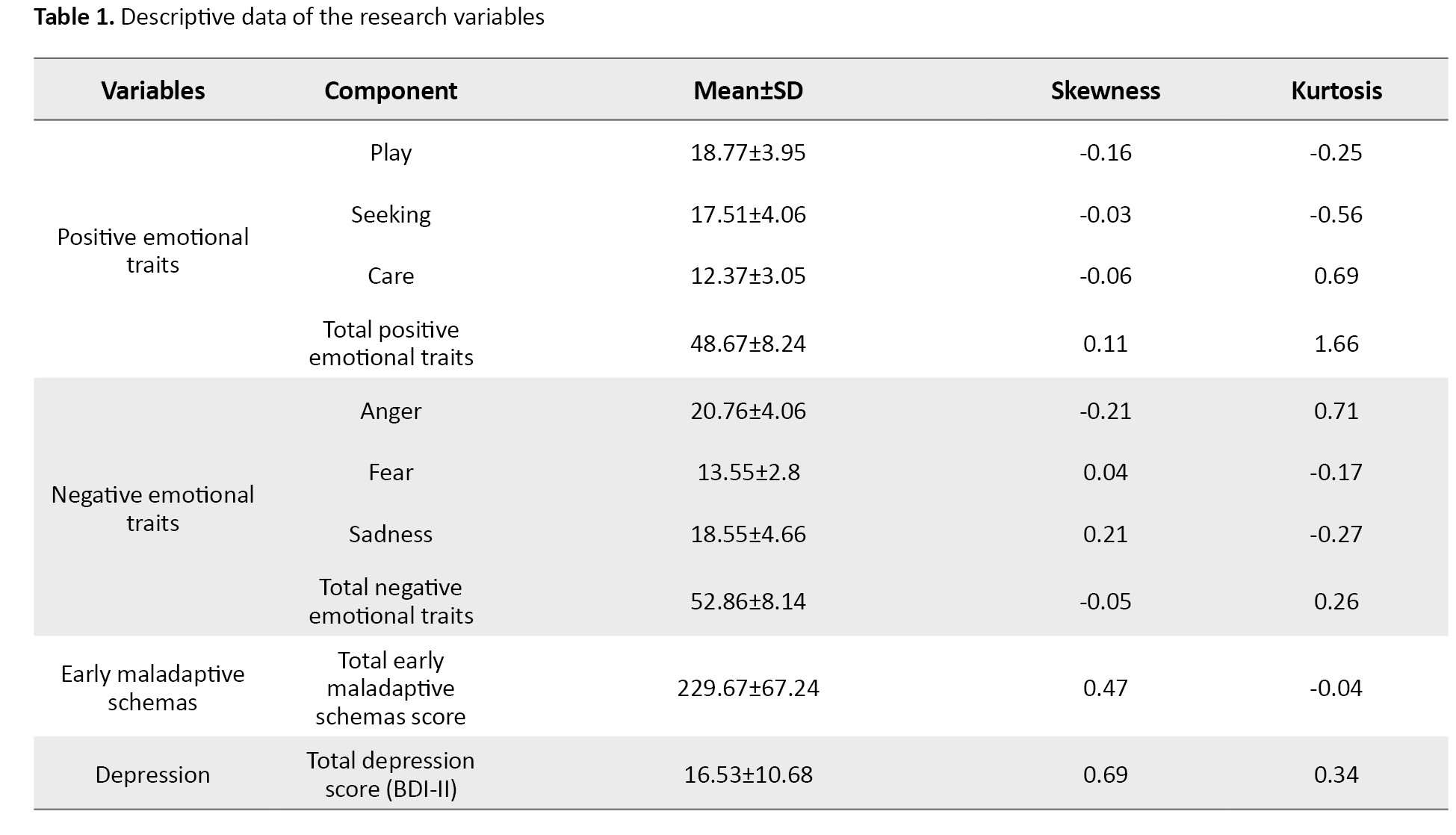
Table 1 presents the means and standard deviations for positive and negative emotional traits, EMSs, and depression scores. Table 2 displays the correlation matrix among the study variables.
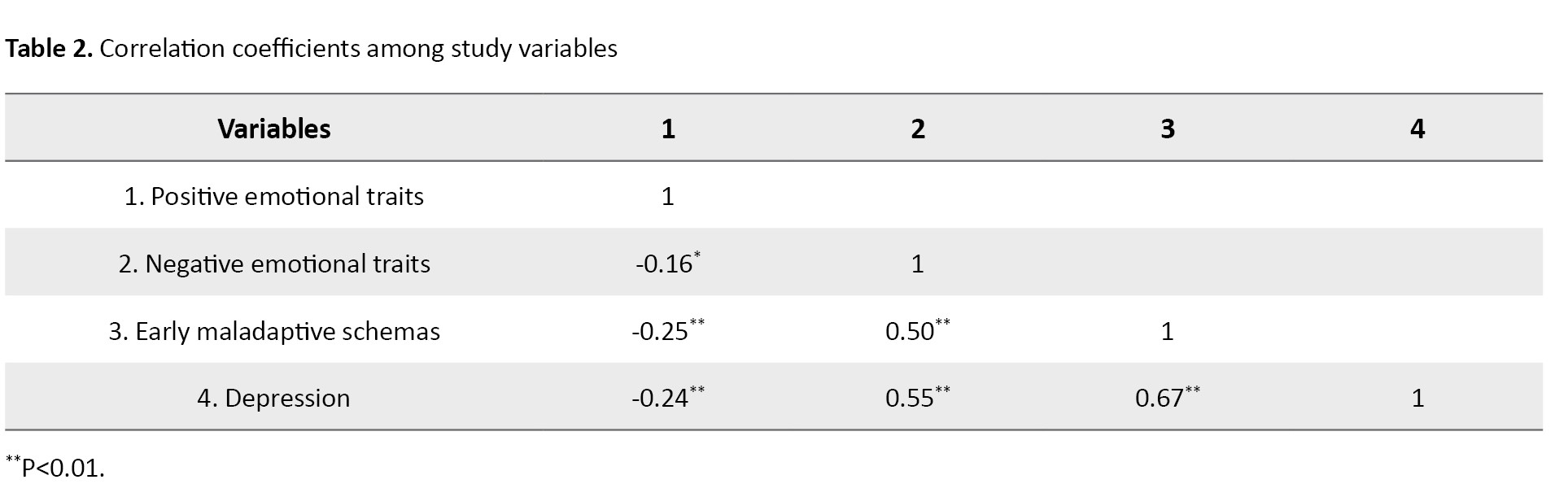
The data in Table 2 indicate that all study variables are significantly correlated. Before evaluating the hypothesized model, the assumptions of SEM were examined. The results showed that the measurement scales were at the interval level and that the variables were normally distributed (skewness <3, kurtosis <10). In addition, the standardized Mardia’s coefficient of multivariate kurtosis (6.15) was below the critical value of p(p+2) for 12 observed variables, confirming multivariate normality—a key assumption in SEM analyses [13].
Furthermore, the assumption of no multicollinearity was met, as the VIF values for positive emotional traits, negative emotional traits, and EMSs were 1.07, 1.34, and 1.39, respectively, and their tolerance values were 0.93, 0.75, and 0.72—indicating acceptable ranges. The assumption of independent errors was also supported, as the Durbin-Watson test yielded a value of 1.91, which falls within the acceptable range (1.5 to 2.5).
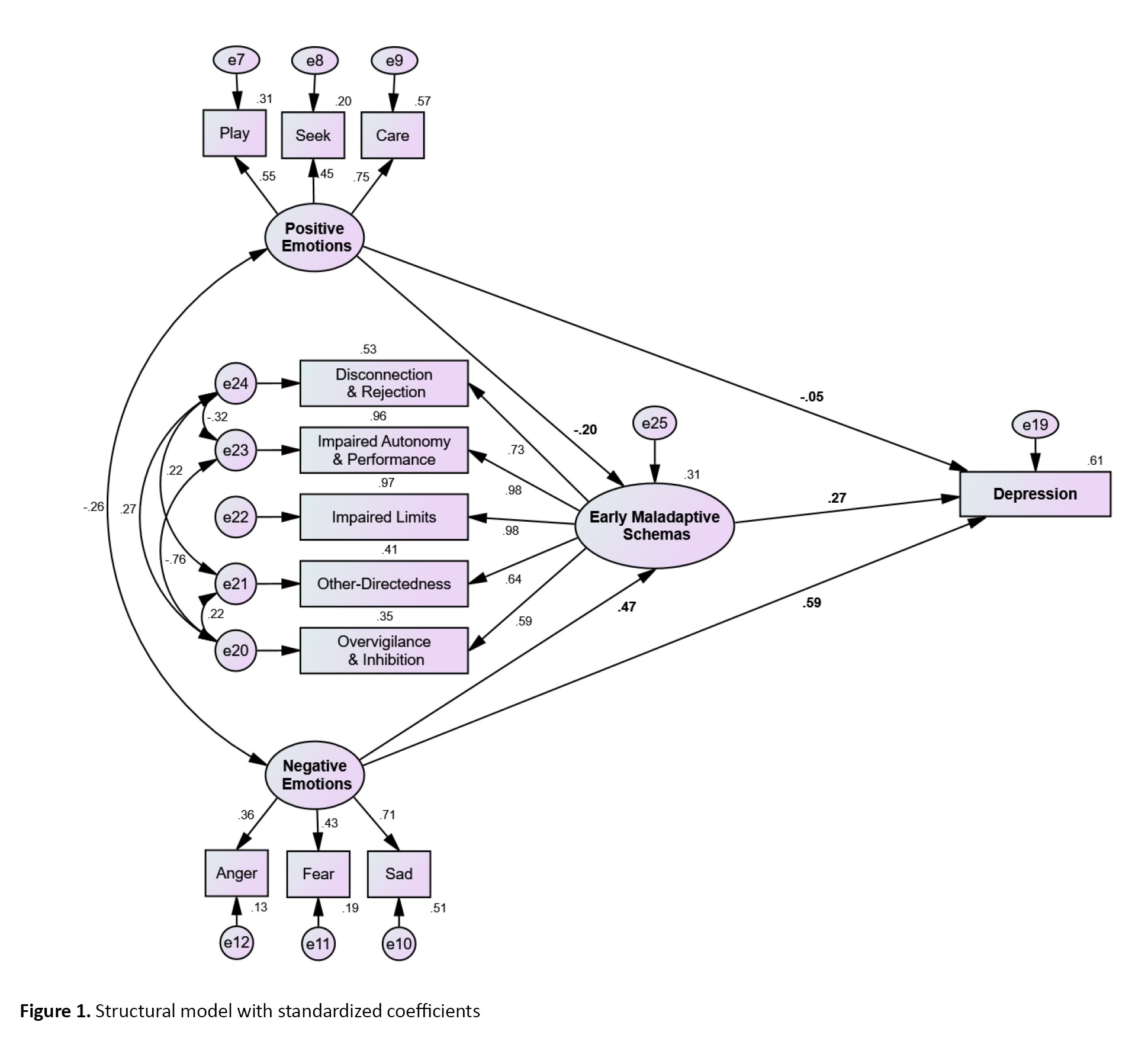
Given that all assumptions were satisfied, SEM was used to analyze the data. The results indicated that the initial measurement model showed poor fit to the data and required modification. After applying the suggested modifications in AMOS, such as correlating the error terms of related indicators, the revised model demonstrated an acceptable fit. Figure 1 presents the final structural model with standardized coefficients.
Adolescence is a critical developmental period marking the transition from childhood to adulthood and is characterized by emotional instability, evolving autonomy, and increased parent-child conflicts [1]. During this stage, adolescents develop more advanced cognitive abilities, including abstract thinking, explore their emerging sense of self and identity, and engage in comparisons regarding lifestyles and values as part of their psychosocial development [2]. Alongside these developmental changes, the risk of major depressive disorder (MDD) increases considerably, with depression typically emerging in mid-adolescence and often following a recurrent course [3]. Depressive symptoms during this period are linked to academic difficulties, impaired social functioning, substance use, and suicidal behaviors, with well-established risk factors such as family history, gender, maltreatment, chronic illness, emotional dispositions, and early maladaptive schemas (EMSs) [4].
Primary emotional traits—defined as evolutionarily rooted, biologically based affective tendencies such as sadness, fear, anger, seeking, and play—have been strongly associated with adolescent depression [4]. Empirical evidence indicates that heightened sadness, fear, and anger, accompanied by reduced seeking and play behaviors, significantly elevate depressive vulnerability. Among these, sadness appears to be the most strongly linked to depressive symptomatology [4]. Inadequate caregiving systems further diminish social engagement and emotional support, contributing to increased social isolation [5]. Neurobiological findings also suggest that fear- and distress-related processes are associated with reduced activation of reward circuitry, particularly during anticipation of positive social outcomes, thereby intensifying motivational deficits and negative affect [6]. Collectively, primary emotional traits may represent key vulnerability factors for depression by amplifying negative emotions, undermining motivation, and impairing social bonding [4].
EMSs are stable and pervasive cognitive-emotional patterns that often arise from adverse childhood experiences. These schemas significantly contribute to the emergence of depressive and anxiety symptoms during adolescence [7]. Rooted in Young schema theory, they can distort how individuals process information, intensify negative emotions, and are strongly linked to depression, anxiety, and difficulties in interpersonal relationships among adolescents and young adults [8]. The persistence of these schemas is reinforced through long-standing emotional-cognitive dysfunctions, which contribute to the stability of psychopathology across development [9].
Despite substantial evidence linking both primary emotional traits and EMSs to depressive symptoms, previous studies have not examined how these constructs interact within a unified framework. In particular, no study has evaluated whether EMSs mediate the relationship between primary emotional traits and adolescent depression, nor has research applied structural equation modeling (SEM) to test this mechanism during adolescence. This study investigates whether EMSs mediate the relationship between primary emotional traits and depressive symptoms in adolescents, addressing this critical gap in the existing literature.
Materials and Methods
This study employed a correlational design and targeted all male and female high school students (grades 10-12) aged 14–19 years living in Isfahan City, Iran. The minimum sample size was determined based on the recommended 1:15 ratio of participants to variables. Considering the 15 subscales of EMSs, 6 subscales of primary emotional traits, and the depression scale (a total of 22 subscales), a minimum of 330 participants was required.
A multistage cluster sampling method was used. First, permission was obtained from the Isfahan Department of Education. Then, 6 high schools (3 girls ‘and 3 boys’) were randomly selected from the city’s list of all public high schools. In the next stage, one class was randomly chosen from each selected school, and all students in those classes were invited to participate. The study objectives were explained to the students, and voluntary participation, confidentiality, and the right to withdraw at any time were emphasized. After excluding incomplete or invalid questionnaires, 253 students’ data remained and were included in the analyses.
The inclusion criteria consisted of being a high school student in grades 10–12, aged 14-19 years, and willingness to participate and complete the questionnaires. The exclusion criteria included incomplete questionnaires and withdrawal from participation at any stage.
Data analysis was performed using SPSS software, version 24 and AMOS software, version 24. SEM was used to examine the measurement and structural models. Model fit was evaluated using commonly recommended indices, including χ²/df, comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean square error approximation (RMSEA).
The following questionnaires were used to collect data.
Brief affective neuroscience personality scale (BANPS):
The BANPS assesses 6 primary emotional traits (seeking, care, play, anger, fear, and sadness) based on Panksepp’s affective neuroscience model. Responses are rated on a 5-point Likert scale. In previous research, the subscales demonstrated Cronbach α values ranging from 0.73 to 0.81 [10]. In the present study, the Cronbach α was 0.59 for positive emotional traits (seeking, care, play), 0.65 for negative traits (anger, fear, sadness), and 0.61 for the total scale, indicating relatively low internal consistency, which should be considered a limitation.
Composite scores for positive and negative emotional traits were based on theoretical considerations: seeking, care, and play were combined as positive traits, reflecting approach-related and affiliative emotional systems, while anger, fear, and sadness were combined as negative traits, reflecting avoidance-related and distress emotional systems [5].
Young schema questionnaire (YSQ)– short form (2003):
The YSQ is a 75-item instrument, rated on a 6-point Likert scale, that assesses 15 EMSs across five domains. The YSQ-SF has been extensively used in both clinical and research contexts and has demonstrated excellent reliability and validity in recent psychometric studies [11]. In the present study, the Cronbach α was 0.9 for the disconnection and rejection domain, 0.86 for impaired autonomy and performance, 0.78 for impaired limits, 0.80 for other-directedness, and 0.79 for hypervigilance and inhibition, with an overall reliability of 0.95 across all schemas.
In this study, EMSs were further categorized as follows: fundamental schemas, comprising the domains of disconnection and rejection, impaired autonomy and performance, and impaired limits; and compensatory schemas, comprising the domains of other-directedness and hypervigilance and inhibition. Scores for each domain were obtained from participants’ responses on the YSQ-SF.
Beck depression inventory-II (BDI-II)
The BDI-II is a 21-item multiple-choice instrument. It is designed to assess the severity of depressive symptoms, with scores ranging from 0 to 63, classified into 4 levels from minimal to severe. The BDI‑II is widely used in both research and clinical practice and demonstrates excellent psychometric properties, including high internal consistency (α≈0.9) and adequate test re-test reliability. Recent studies have confirmed that this tool exhibits strong validity and reliability, making it suitable for assessing depression across diverse populations [12]. In the current study, the Cronbach α was 0.9.
In this study, adolescent depression was defined as the total score obtained by participants on the BDI-II.
Results
A total of 253 individuals participated in this study. During the data screening process (to ensure multivariate normality), 2 participants were excluded. Thus, the final sample consisted of 251 participants. Among them, 195 participants (77.7%) were female, and 56(22.3%) were male. The mean and standard deviation of participants’ age were as follows: for girls, 16.42±0.83 years; for boys, 16.25±1.16 years; and for the total sample, 16.38±0.91 years. Table 1 presents the Mean±SD, skewness, and kurtosis for the study variables.
Table 1 presents the means and standard deviations for positive and negative emotional traits, EMSs, and depression scores. Table 2 displays the correlation matrix among the study variables.
The data in Table 2 indicate that all study variables are significantly correlated. Before evaluating the hypothesized model, the assumptions of SEM were examined. The results showed that the measurement scales were at the interval level and that the variables were normally distributed (skewness <3, kurtosis <10). In addition, the standardized Mardia’s coefficient of multivariate kurtosis (6.15) was below the critical value of p(p+2) for 12 observed variables, confirming multivariate normality—a key assumption in SEM analyses [13].
Furthermore, the assumption of no multicollinearity was met, as the VIF values for positive emotional traits, negative emotional traits, and EMSs were 1.07, 1.34, and 1.39, respectively, and their tolerance values were 0.93, 0.75, and 0.72—indicating acceptable ranges. The assumption of independent errors was also supported, as the Durbin-Watson test yielded a value of 1.91, which falls within the acceptable range (1.5 to 2.5).
Given that all assumptions were satisfied, SEM was used to analyze the data. The results indicated that the initial measurement model showed poor fit to the data and required modification. After applying the suggested modifications in AMOS, such as correlating the error terms of related indicators, the revised model demonstrated an acceptable fit. Figure 1 presents the final structural model with standardized coefficients.
As shown in Figure 1, the hypothesized model proposed that EMSs mediate the relationship between primary emotional traits (positive and negative) and depression. Model fit indices are presented in Table 3.
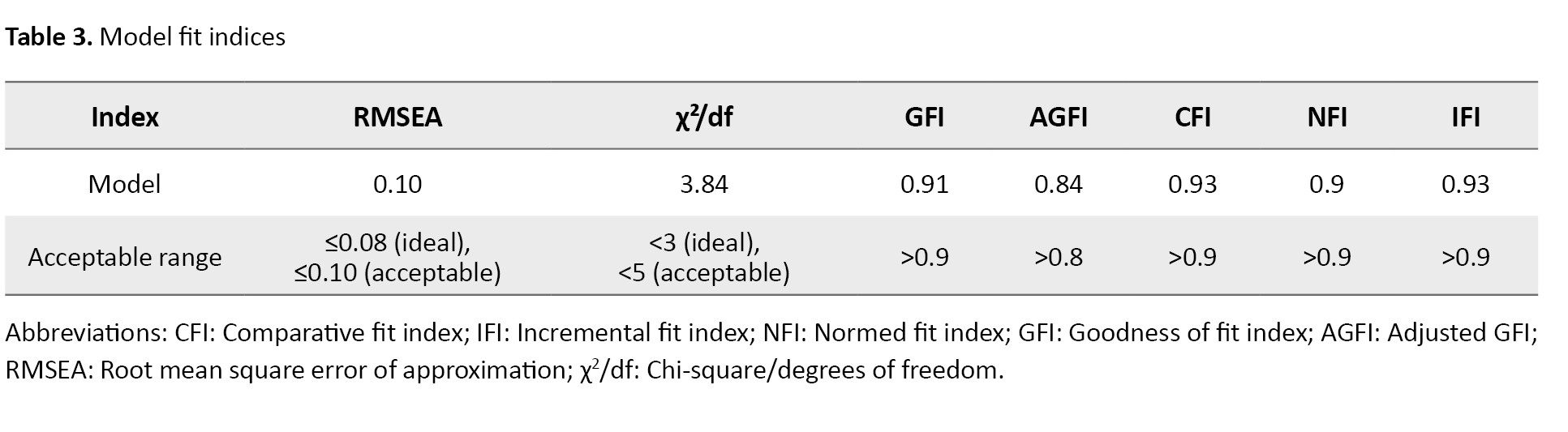
The indices reported in Table 3 indicate an overall acceptable but marginal fit of the proposed model. Specifically, the values of the goodness-of-fit index (GFI) and the adjusted GFI (AGFI), as absolute fit indices, as well as the values of the CFI, normed fit index (NFI), and incremental fit index (IFI), as comparative fit indices, are within acceptable ranges. The RMSEA value (0.10) exceeds the recommended threshold for good fit, indicating borderline model fit rather than good fit. Similarly, the χ²/df value (3.84) is marginal. Taken together, these results suggest that although the model does not show an optimal fit, it demonstrates a reasonable and acceptable level of fit and was therefore retained for interpretation.
Table 4 presents the direct effects of the predictor variables on the mediator and outcome variables.
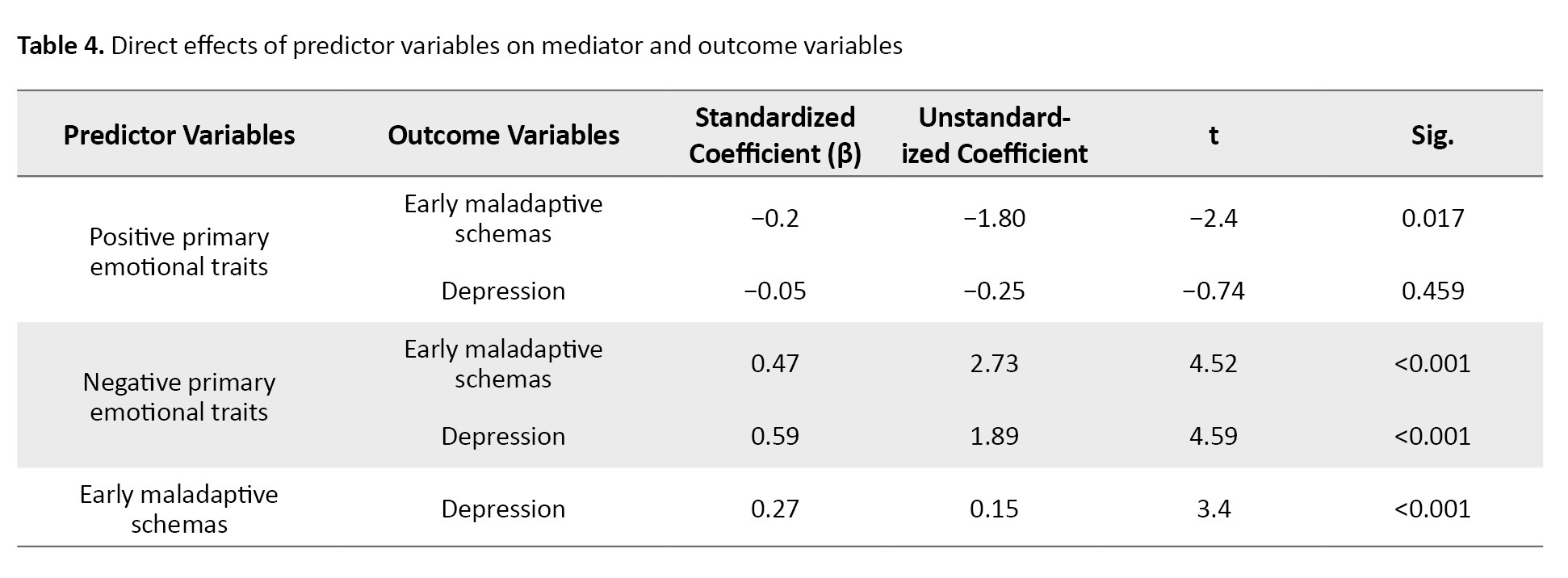
As shown in Table 4, the direct effect of positive primary emotional traits on EMSs is negative and statistically significant (β=−0.20, P=0.017). However, its direct effect on depression is not significant (β=−0.05, P=0.459). On the other hand, negative primary emotional traits have positive and statistically significant effects on both EMSs (β=0.47, P<0.001) and depression (β=0.59, P<0.001). Furthermore, EMSs also have a positive and statistically significant direct effect on depression (β=0.27, P<0.001).
Table 5 presents the results of the indirect effects of the predictor variables on the outcome variable via the mediator variable, based on bootstrap resampling.
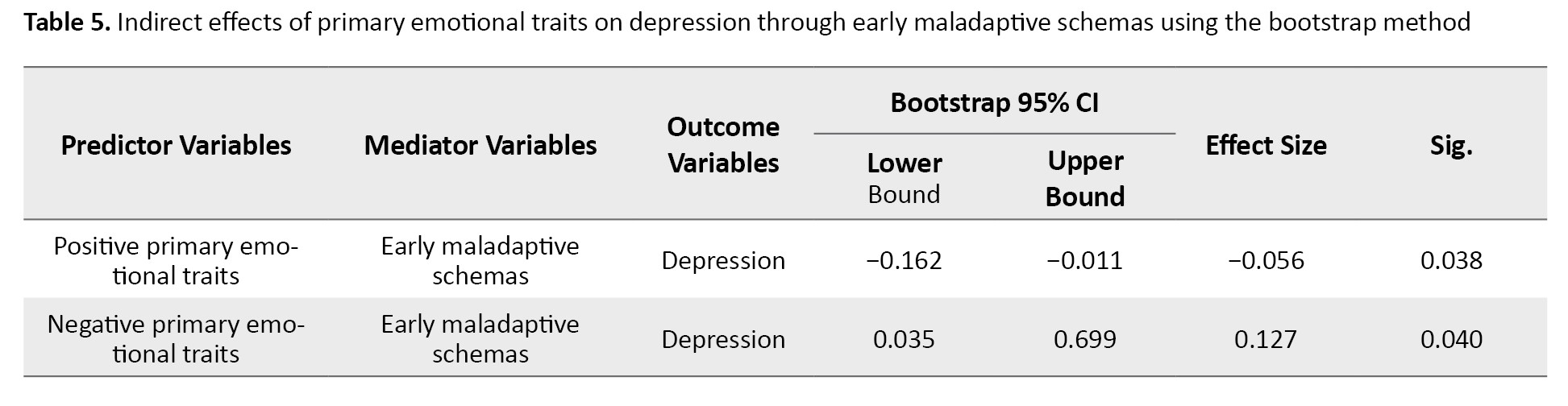
As reported in Table 5, the indirect effect of positive primary emotional traits on depression through EMSs is negative and statistically significant (β=−0.06, P=0.038), with the 95% bootstrap confidence interval (CI) [−0.162%, −0.011%] not including zero. Similarly, the indirect effect of negative primary emotional traits on depression through EMSs is positive and statistically significant (β=0.13, P=0.040), with its 95% bootstrap CI [0.035%, 0.699%] excluding zero. These results indicate that EMSs mediate the relationships between both positive and negative primary emotional traits and depression.
Overall, the findings of the present study indicate that positive primary emotional traits do not have a significant direct effect on depression; however, they indirectly predict depression through EMSs. In contrast, negative primary emotional traits positively and significantly predict depression both directly and indirectly through EMSs.
Discussion
The present study examined the relationships between primary emotional traits and depressive symptoms in adolescents, as well as the mediating role of EMSs in a sample of high school students in Isfahan, Iran. The main findings can be summarized as follows: positive primary emotional traits were negatively associated with EMSs but showed no significant direct association with depression; negative primary emotional traits were positively and significantly linked to both EMSs and depression; EMSs themselves had a significant positive association with depressive symptoms; and both positive and negative primary emotional traits exhibited significant indirect associations with depression through EMSs.
Positive primary emotional traits were significantly and negatively associated with EMSs (β=−0.20, P<0.05). This finding suggests that adolescents with higher activation of basic positive emotional systems (seeking, care, play, lust) tend to develop fewer maladaptive cognitive patterns. These positive primary emotional traits appear to act as protective factors against the internalization of early adverse experiences into rigid, negative core beliefs, consistent with affective neuroscience research indicating that individual differences in primary emotional systems, such as seeking, play, and care, relate to adaptive affective functioning and lower levels of psychopathology [14]. As suggested by affective neuroscience, active positive emotional systems promote safe, exploratory, and prosocial behaviors, which may buffer the formation of maladaptive schemas even in the presence of environmental stressors [14]. This result is consistent with previous studies demonstrating that higher levels of positive primary emotional traits are associated with lower maladaptive schemas and better overall mental health outcomes in both clinical and non-clinical adolescent samples [15, 16].
Negative primary emotional traits were strongly positively associated with EMSs (β=0.47, P<0.01). Adolescents with more chronically active negative systems (fear, anger, sadness) tend to perceive early adverse experiences as more threatening or rejecting, which in turn fosters the development of schemas such as mistrust/abuse, vulnerability to harm, emotional deprivation, and social isolation [17]. This pattern aligns with Young schema theory and Panksepp affective neuroscience framework, both of which emphasize the critical role of innate emotional temperament in amplifying or attenuating the impact of childhood adversity on core belief formation [18, 19]. Numerous studies have similarly reported that enduring negative emotionality, particularly when combined with early maltreatment or dysfunctional parenting, significantly predicts higher levels of maladaptive schemas in adolescence and young adulthood [18, 19].
EMSs were positively and significantly associated with depressive symptoms (β=0.27, P<0.01). These findings are consistent with extensive evidence suggesting that negative core beliefs about the self, others, and the future constitute key cognitive vulnerabilities in the onset and persistence of depression [20, 21]. Once activated, these schemas trigger automatic negative thoughts, self-criticism, hopelessness, and feelings of worthlessness—processes that directly contribute to depressive symptomatology [20-22]. In adolescence, a developmental period characterized by heightened sensitivity to social evaluation and identity formation, the presence of severe EMSs appears to have particularly detrimental effects on emotional well-being [22, 7].
With respect to direct associations with depression, positive primary emotional traits showed no statistically significant association (β=−0.05, P>0.05), whereas negative primary emotional traits showed a strong positive association (β=0.59, P<0.01). The absence of a direct protective effect of positive primary emotional traits suggests that their beneficial influence on adolescent mental health is not automatic; rather, it may be shaped by cognitive mediators (such as schemas and emotion regulation strategies) and developmental contexts, including early caregiver relationships and attachment security [14, 23]. In contrast, chronically active negative primary emotional traits seem capable of contributing directly to depressive states by sustaining negative affect, reducing hedonic capacity, and impairing motivation—mechanisms linked to downregulation of dopaminergic reward circuits and prefrontal-limbic dysregulation [24]. These results converge with longitudinal and cross-sectional studies indicating that high negative emotionality in childhood and adolescence is among the strongest temperament-based predictors of later emotional disorders, including depressive episodes [25].
A central finding of this study is the presence of significant indirect associations of both positive and negative primary emotional traits with depression through EMSs. Specifically, positive primary emotional traits were linked to lower levels of depression indirectly via reduced EMSs (β=−0.06, P<0.05). In contrast, negative primary emotional traits were associated with higher depression both directly and indirectly through elevated EMSs (β=0.13, P<0.05 for the indirect path). These contrasting pathways illustrate that positive primary emotional traits primarily exert their protective role by preventing or minimizing maladaptive cognitive structures. In contrast, negative primary emotional traits operate through dual channels—directly via sustained negative affect and indirectly by intensifying schema formation [26-29]. This mediated model highlights EMSs as a key cognitive mechanism that translates biologically rooted emotional tendencies into clinical-level depressive symptoms in adolescence.
In summary, positive primary emotional traits showed no significant direct association with depression but a significant negative indirect association through lower EMSs. Negative primary emotional traits, however, displayed both a strong positive direct association and a significant positive indirect association with depression via higher EMSs. EMSs themselves were significantly and positively linked to depressive symptoms. These findings emphasize the clinical importance of identifying and modifying EMSs, especially in adolescents exhibiting pronounced negative primary emotional traits, and support the integration of schema-focused interventions in prevention and treatment programs for adolescent depression.
These findings underscore the critical role of EMSs as a key cognitive–emotional mechanism through which biologically rooted emotional dispositions influence depressive symptomatology during adolescence. Adolescents characterized by heightened negative emotional traits such as sadness, fear, and anger may be particularly vulnerable to developing maladaptive schemas, which in turn intensify depressive symptoms.
From a clinical perspective, the results highlight the importance of early identification and modification of maladaptive schemas, especially in adolescents with pronounced negative primary emotional traits. Integrating schema-focused interventions into prevention and treatment programs may help reduce cognitive vulnerability and mitigate the progression of depressive symptoms during this sensitive developmental period. Overall, the present findings contribute to a more integrative understanding of the interplay between primary emotional systems and cognitive vulnerabilities in adolescent depression.
Conclusion
In conclusion, the study’s findings support the hypothesized mediating role of EMSs in the relationship between primary emotional traits and adolescent depression. Negative primary emotional traits showed both significant direct and indirect positive associations with depressive symptoms via EMSs. In contrast, positive traits were indirectly associated with lower depression through reduced maladaptive schemas. These results underscore the importance of addressing cognitive vulnerabilities in adolescents and provide theoretical and practical guidance for developing preventive and therapeutic interventions aimed at reducing depressive symptoms in this population.
Limitation and future direction
One of the primary limitations of the present study is its correlational, cross-sectional design, which prevents the establishment of causal relationships among primary emotional traits, EMSs, and adolescent depression. Additionally, the reliance on self-report questionnaires may have introduced response biases such as social desirability or inaccurate self-assessment. The sample was predominantly female (77%), which may limit the generalizability of the findings to male adolescents, given potential gender differences in emotional processing, maladaptive schemas, and depressive symptoms. Furthermore, participants were recruited exclusively from high school students in Isfahan, which may limit the generalizability of the results to adolescents from other areas or backgrounds.
Future studies should consider longitudinal or experimental designs to examine better the causal pathways among emotional traits, schemas, and depression. Moreover, incorporating qualitative methods, multi-informant reports (e.g. parents, teachers), and clinical interviews could enhance the validity of the findings. Expanding the sample to include diverse age groups, geographical regions, and cultural backgrounds would also provide a more comprehensive understanding of these psychological mechanisms and support the development of tailored interventions for adolescent mental health.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of the University of Tabriz, Tabriz, Iran (Code: IR.TABRIZU.REC.1404.023). Before participation, informed consent was obtained from all participants after explaining the study’s objectives, confidentiality of data and their right to withdraw at any time without any consequences.
Funding
This study was extracted from the master's thesis of Leila Ebrahimi varzaneh, approved by the Department of psychology Faculty of Educational Sciences and psycholo-gy, University of Tabriz, Tabriz, Iran.
Authors contributions
Conceptualization: Khalil Esmaeilpour and Leila Ebrahimi Varzaneh; Methodology, supervision, review and editing: Khalil Esmaeilpour and Zeinab Khanjani; Data curation, formal analysis, investigation, and writing the original draft: Leila Ebrahimi Varzaneh; Validation: Zeinab Khanjani.
Conflict of interest
The author declared no conflict of interest.
Acknowledgements
The authors would like to express our sincere gratitude to all the students who kindly participated in this study by completing the questionnaires. Their time, honesty, and cooperation were essential to the success of this research.
The indices reported in Table 3 indicate an overall acceptable but marginal fit of the proposed model. Specifically, the values of the goodness-of-fit index (GFI) and the adjusted GFI (AGFI), as absolute fit indices, as well as the values of the CFI, normed fit index (NFI), and incremental fit index (IFI), as comparative fit indices, are within acceptable ranges. The RMSEA value (0.10) exceeds the recommended threshold for good fit, indicating borderline model fit rather than good fit. Similarly, the χ²/df value (3.84) is marginal. Taken together, these results suggest that although the model does not show an optimal fit, it demonstrates a reasonable and acceptable level of fit and was therefore retained for interpretation.
Table 4 presents the direct effects of the predictor variables on the mediator and outcome variables.
As shown in Table 4, the direct effect of positive primary emotional traits on EMSs is negative and statistically significant (β=−0.20, P=0.017). However, its direct effect on depression is not significant (β=−0.05, P=0.459). On the other hand, negative primary emotional traits have positive and statistically significant effects on both EMSs (β=0.47, P<0.001) and depression (β=0.59, P<0.001). Furthermore, EMSs also have a positive and statistically significant direct effect on depression (β=0.27, P<0.001).
Table 5 presents the results of the indirect effects of the predictor variables on the outcome variable via the mediator variable, based on bootstrap resampling.
As reported in Table 5, the indirect effect of positive primary emotional traits on depression through EMSs is negative and statistically significant (β=−0.06, P=0.038), with the 95% bootstrap confidence interval (CI) [−0.162%, −0.011%] not including zero. Similarly, the indirect effect of negative primary emotional traits on depression through EMSs is positive and statistically significant (β=0.13, P=0.040), with its 95% bootstrap CI [0.035%, 0.699%] excluding zero. These results indicate that EMSs mediate the relationships between both positive and negative primary emotional traits and depression.
Overall, the findings of the present study indicate that positive primary emotional traits do not have a significant direct effect on depression; however, they indirectly predict depression through EMSs. In contrast, negative primary emotional traits positively and significantly predict depression both directly and indirectly through EMSs.
Discussion
The present study examined the relationships between primary emotional traits and depressive symptoms in adolescents, as well as the mediating role of EMSs in a sample of high school students in Isfahan, Iran. The main findings can be summarized as follows: positive primary emotional traits were negatively associated with EMSs but showed no significant direct association with depression; negative primary emotional traits were positively and significantly linked to both EMSs and depression; EMSs themselves had a significant positive association with depressive symptoms; and both positive and negative primary emotional traits exhibited significant indirect associations with depression through EMSs.
Positive primary emotional traits were significantly and negatively associated with EMSs (β=−0.20, P<0.05). This finding suggests that adolescents with higher activation of basic positive emotional systems (seeking, care, play, lust) tend to develop fewer maladaptive cognitive patterns. These positive primary emotional traits appear to act as protective factors against the internalization of early adverse experiences into rigid, negative core beliefs, consistent with affective neuroscience research indicating that individual differences in primary emotional systems, such as seeking, play, and care, relate to adaptive affective functioning and lower levels of psychopathology [14]. As suggested by affective neuroscience, active positive emotional systems promote safe, exploratory, and prosocial behaviors, which may buffer the formation of maladaptive schemas even in the presence of environmental stressors [14]. This result is consistent with previous studies demonstrating that higher levels of positive primary emotional traits are associated with lower maladaptive schemas and better overall mental health outcomes in both clinical and non-clinical adolescent samples [15, 16].
Negative primary emotional traits were strongly positively associated with EMSs (β=0.47, P<0.01). Adolescents with more chronically active negative systems (fear, anger, sadness) tend to perceive early adverse experiences as more threatening or rejecting, which in turn fosters the development of schemas such as mistrust/abuse, vulnerability to harm, emotional deprivation, and social isolation [17]. This pattern aligns with Young schema theory and Panksepp affective neuroscience framework, both of which emphasize the critical role of innate emotional temperament in amplifying or attenuating the impact of childhood adversity on core belief formation [18, 19]. Numerous studies have similarly reported that enduring negative emotionality, particularly when combined with early maltreatment or dysfunctional parenting, significantly predicts higher levels of maladaptive schemas in adolescence and young adulthood [18, 19].
EMSs were positively and significantly associated with depressive symptoms (β=0.27, P<0.01). These findings are consistent with extensive evidence suggesting that negative core beliefs about the self, others, and the future constitute key cognitive vulnerabilities in the onset and persistence of depression [20, 21]. Once activated, these schemas trigger automatic negative thoughts, self-criticism, hopelessness, and feelings of worthlessness—processes that directly contribute to depressive symptomatology [20-22]. In adolescence, a developmental period characterized by heightened sensitivity to social evaluation and identity formation, the presence of severe EMSs appears to have particularly detrimental effects on emotional well-being [22, 7].
With respect to direct associations with depression, positive primary emotional traits showed no statistically significant association (β=−0.05, P>0.05), whereas negative primary emotional traits showed a strong positive association (β=0.59, P<0.01). The absence of a direct protective effect of positive primary emotional traits suggests that their beneficial influence on adolescent mental health is not automatic; rather, it may be shaped by cognitive mediators (such as schemas and emotion regulation strategies) and developmental contexts, including early caregiver relationships and attachment security [14, 23]. In contrast, chronically active negative primary emotional traits seem capable of contributing directly to depressive states by sustaining negative affect, reducing hedonic capacity, and impairing motivation—mechanisms linked to downregulation of dopaminergic reward circuits and prefrontal-limbic dysregulation [24]. These results converge with longitudinal and cross-sectional studies indicating that high negative emotionality in childhood and adolescence is among the strongest temperament-based predictors of later emotional disorders, including depressive episodes [25].
A central finding of this study is the presence of significant indirect associations of both positive and negative primary emotional traits with depression through EMSs. Specifically, positive primary emotional traits were linked to lower levels of depression indirectly via reduced EMSs (β=−0.06, P<0.05). In contrast, negative primary emotional traits were associated with higher depression both directly and indirectly through elevated EMSs (β=0.13, P<0.05 for the indirect path). These contrasting pathways illustrate that positive primary emotional traits primarily exert their protective role by preventing or minimizing maladaptive cognitive structures. In contrast, negative primary emotional traits operate through dual channels—directly via sustained negative affect and indirectly by intensifying schema formation [26-29]. This mediated model highlights EMSs as a key cognitive mechanism that translates biologically rooted emotional tendencies into clinical-level depressive symptoms in adolescence.
In summary, positive primary emotional traits showed no significant direct association with depression but a significant negative indirect association through lower EMSs. Negative primary emotional traits, however, displayed both a strong positive direct association and a significant positive indirect association with depression via higher EMSs. EMSs themselves were significantly and positively linked to depressive symptoms. These findings emphasize the clinical importance of identifying and modifying EMSs, especially in adolescents exhibiting pronounced negative primary emotional traits, and support the integration of schema-focused interventions in prevention and treatment programs for adolescent depression.
These findings underscore the critical role of EMSs as a key cognitive–emotional mechanism through which biologically rooted emotional dispositions influence depressive symptomatology during adolescence. Adolescents characterized by heightened negative emotional traits such as sadness, fear, and anger may be particularly vulnerable to developing maladaptive schemas, which in turn intensify depressive symptoms.
From a clinical perspective, the results highlight the importance of early identification and modification of maladaptive schemas, especially in adolescents with pronounced negative primary emotional traits. Integrating schema-focused interventions into prevention and treatment programs may help reduce cognitive vulnerability and mitigate the progression of depressive symptoms during this sensitive developmental period. Overall, the present findings contribute to a more integrative understanding of the interplay between primary emotional systems and cognitive vulnerabilities in adolescent depression.
Conclusion
In conclusion, the study’s findings support the hypothesized mediating role of EMSs in the relationship between primary emotional traits and adolescent depression. Negative primary emotional traits showed both significant direct and indirect positive associations with depressive symptoms via EMSs. In contrast, positive traits were indirectly associated with lower depression through reduced maladaptive schemas. These results underscore the importance of addressing cognitive vulnerabilities in adolescents and provide theoretical and practical guidance for developing preventive and therapeutic interventions aimed at reducing depressive symptoms in this population.
Limitation and future direction
One of the primary limitations of the present study is its correlational, cross-sectional design, which prevents the establishment of causal relationships among primary emotional traits, EMSs, and adolescent depression. Additionally, the reliance on self-report questionnaires may have introduced response biases such as social desirability or inaccurate self-assessment. The sample was predominantly female (77%), which may limit the generalizability of the findings to male adolescents, given potential gender differences in emotional processing, maladaptive schemas, and depressive symptoms. Furthermore, participants were recruited exclusively from high school students in Isfahan, which may limit the generalizability of the results to adolescents from other areas or backgrounds.
Future studies should consider longitudinal or experimental designs to examine better the causal pathways among emotional traits, schemas, and depression. Moreover, incorporating qualitative methods, multi-informant reports (e.g. parents, teachers), and clinical interviews could enhance the validity of the findings. Expanding the sample to include diverse age groups, geographical regions, and cultural backgrounds would also provide a more comprehensive understanding of these psychological mechanisms and support the development of tailored interventions for adolescent mental health.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of the University of Tabriz, Tabriz, Iran (Code: IR.TABRIZU.REC.1404.023). Before participation, informed consent was obtained from all participants after explaining the study’s objectives, confidentiality of data and their right to withdraw at any time without any consequences.
Funding
This study was extracted from the master's thesis of Leila Ebrahimi varzaneh, approved by the Department of psychology Faculty of Educational Sciences and psycholo-gy, University of Tabriz, Tabriz, Iran.
Authors contributions
Conceptualization: Khalil Esmaeilpour and Leila Ebrahimi Varzaneh; Methodology, supervision, review and editing: Khalil Esmaeilpour and Zeinab Khanjani; Data curation, formal analysis, investigation, and writing the original draft: Leila Ebrahimi Varzaneh; Validation: Zeinab Khanjani.
Conflict of interest
The author declared no conflict of interest.
Acknowledgements
The authors would like to express our sincere gratitude to all the students who kindly participated in this study by completing the questionnaires. Their time, honesty, and cooperation were essential to the success of this research.
References
- Papalia DE, Feldman RD, Olds SW. Human development [A. Hayat, D. Ghahestani, H. Sohrabi, S. Naghshbandi, F. & Davarpanah, H. Yans, Persian Trans]. Tehran: Roshd Publication; 2025. [Link]
- Pfeifer JH, Berkman ET. The development of self and identity in adolescence: Neural evidence and implications for a value-based choice perspective on motivated behavior. Child Development Perspectives. 2018; 12(3):158-64. [DOI:10.1111/cdep.12279] [PMID]
- Bigham Laleabadi E, Narimani M, Hajimiradi R. [Meta-analysis of behavioral activation therapy on adolescent depression (Persian)]. Quarterly Journal of Psychological Methods and Models. 2022; 13(47):161-74. [Link]
- Brienza L, Zennaro A, Vitolo E, Andò A. Affective neuroscience personality scale (ANPS) and clinical implications: A systematic review. Journal of Affective Disorders. 2023; 320:178-95. [DOI:10.1016/j.jad.2022.09.104] [PMID]
- Montag C, Widenhorn-Müller K, Panksepp J, Kiefer M. Individual differences in affective neuroscience personality scale primary emotional traits and depressive tendencies. Comprehensive Psychiatry. 2017; 73:136-42. [DOI:10.1016/j.comppsych.2016.11.007] [PMID]
- Richey AR, Ghane J, Valdespino A, Coffman MC, Strege MV, White SW, et al. Spatiotemporal dissociation of brain activity underlying threat and reward in social anxiety disorder. Social Cognitive and Affective Neuroscience. 2016; 12:81-94. [DOI:10.1093/scan/nsw149] [PMID]
- Ahrnberg H, Lindblom J, Kaltiala R, Karukivi M. Early maladaptive schemas, depression and anxiety in adolescent psychiatric outpatients. Behavioural and Cognitive Psychotherapy. 2025; 53(2):206-10. [DOI:10.1017/S1352465824000432] [PMID]
- Tariq A, Quayle E, Lawrie SM, Reid C, Chan SWY. Relationship between early maladaptive schemas and anxiety in adolescence and young adulthood: A systematic review and meta-analysis. Journal of Affective Disorders. 2021; 295:1462-73. [DOI:10.1016/j.jad.2021.09.031] [PMID]
- Talarowska M, Wysiadecki G, Chodkiewicz J. Affective neuroscience personality scales and early maladaptive schemas in depressive disorders. International Journal of Environmental Research and Public Health. 2022; 19(13):8062. [DOI:10.3390/ijerph19138062] [PMID]
- Amiri S, Azad-Marzabadi E. Validation of affective neuroscience personality scales in normal populations. Neuropsychiatrie Neuropsychologie. 2017; 12(3):95-100. [DOI:10.5114/nan.2017.71665]
- Gonzalez-Cifuentes CE, Ruiz FJ, Quiceno JM. Psychometric properties of the Young early maladaptive schema questionnaire-short form (YSQ-S3) in Colombia. Behavioral Psychology/Psicología Conductual. 2024; 32(1):65-87. [DOI:10.51668/bp.8324103n]
- Hasan MT, Khan MHA. Psychometric properties of the Bangla version of the Beck Depression Inventory-II with university students in Bangladesh: A cross-sectional study. Health Science Reports. 2025; 8(1):e70280. [DOI:10.1002/hsr2.70280] [PMID]
- Liang J, Bentler PM, Cao Y. Testing multivariate normality for two-level structural equation models. Journal of Multivariate Analysis. 2025; 212:105562. [DOI:10.1016/j.jmva.2025.105562]
- Marengo D, Davis KL, Gradwohl GÖ, Montag C. A meta-analysis on individual differences in primary emotional systems and big five personality traits. Scientific Reports. 2021; 11(1):7453. [DOI:10.1038/s41598-021-84366-8] [PMID]
- Phua DY, Chew CSM. Core features of positive mental health in adolescents and their protective role against psychopathology. Scientific Reports. 2025; 15(1):4228. [DOI:10.1038/s41598-025-88454-x] [PMID]
- Nicol A, Mak AS, Murray K, Walker I, Buckmaster D. The relationships between early maladaptive schemas and youth mental health: A systematic review. Cognitive Therapy and Research. 2020; 44(4):715-51. [DOI:10.1007/s10608-020-10092-6]
- Kim ES, Wilkinson R, Okuzono SS, Chen Y, Shiba K, Cowden RG, et al. Positive affect during adolescence and health and well-being in adulthood: An outcome-wide longitudinal approach. PLoS Medicine. 2024; 21(4):e1004365. [DOI:10.1371/journal.pmed.1004365] [PMID]
- Saarijärvi P, Salmivalli C, Helmi S, Karukivi M. Early maladaptive schemas are associated with self-injury thoughts and behavior in adolescents. BMC Psychiatry. 2023; 23:1-10. [DOI:10.1186/s12888-023-05127-7] [PMID]
- May T, Younan R, Pilkington PD. Adolescent maladaptive schemas and childhood abuse and neglect: A systematic review and meta-analysis. Clinical Psychology and Psychotherapy. 2022; 29(4):1159-73. [DOI:10.1002/cpp.2712] [PMID]
- Wang Y, Gao Y, Liu J, Bai R, Liu X. Reciprocal associations between early maladaptive schemas and depression in adolescence. Child and Adolescent Psychiatry and Mental Health. 2023; 17(1):134. [DOI:10.1186/s13034-023-00682-z] [PMID]
- Young KS, Sandman CF, Craske MG. Positive and negative emotion regulation in adolescence: Links to anxiety and depression. Brain Sciences. 2019; 9(4):76. [DOI:10.3390/brainsci9040076] [PMID]
- Seon Y, Smith-Adcock S. Adolescents’ meaning in life as a resilience factor between bullying victimization and life satisfaction. Children and Youth Services Review. 2023; 148:106875. [DOI:10.1016/j.childyouth.2023.106875]
- Vahedi S, Gargari RB, Gholami S. Mediating role of cognitive emotion regulation strategies on the relationship between attachment styles and emotional problems: A path analysis. Iranian Journal of Psychiatry and Behavioral Sciences. 2016; 10:e4346. [DOI:10.17795/ijpbs-4013]
- Davis KL, Montag C. Selected principles of Pankseppian affective neuroscience. Frontiers in Neuroscience. 2019; 12:1025. [DOI:10.3389/fnins.2018.01025] [PMID]
- Bakken NR, Hannigan LJ, Shadrin A, Hindley G, Ask H, Reichborn-Kjennerud T, et al. Childhood temperamental, emotional, and behavioral characteristics associated with mood and anxiety disorders in adolescence. Acta Psychiatrica Scandinavica. 2023; 147(2):217-28. [DOI:10.1111/acps.13522] [PMID]
- Lumley MN, McArthur BA. Protection from depression following emotional maltreatment: The unique role of positive schemas. International Journal of Cognitive Therapy. 2016; 9(4):327-43. [DOI:10.1521/ijct_2016_09_14]
- Thimm JC, Chang M. Early maladaptive schemas and mental disorders in adulthood: A systematic review and meta-analysis. International Journal of Cognitive Therapy. 2022; 15(4):371-413. [DOI:10.1007/s41811-022-00149-7]
- Bishop A, Younan R, Low J, Pilkington PD. Early maladaptive schemas and depression in adulthood: A systematic review and meta-analysis. Clinical Psychology and Psychotherapy. 2022; 29(1):111-30. [DOI:10.1002/cpp.2630] [PMID]
- Ahmadpanah M, Astinsadaf S, Akhondi A, Haghighi M, Sadeghi Bahmani D, Nazaribadie M, et al. Early maladaptive schemas related to suicide attempts among patients with major depressive disorder. Comprehensive Psychiatry. 2017; 77:71-79. [DOI:10.1016/j.comppsych.2017.05.008] [PMID]
Type of Study: Original Article |
Subject:
Health
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
